Vulvitis: Predisposing Factors, Clinical Manifestations, Diagnosis, and Treatment
Vulvitis refers to vulvar inflammation affecting the labia, clitoris, mons pubis, and vestibule of the vagina. Clinical manifestations, diagnosis, and treatment.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Genital tuberculosis ranks second in prevalence after pulmonary tuberculosis. The disease tends to affect the female genitalia in approximately 1.5–2 % of cases.
It is a specific inflammation of the vaginal mucosa caused by M. tuberculosis. Genital tuberculosis typically develops through hematogenous spread; in rare instances, it may spread via lymphatic pathways.
Complaints
Patients may be concerned about nagging lower abdominal pain, pathological vaginal discharge, vaginal bleeding, or infertility.
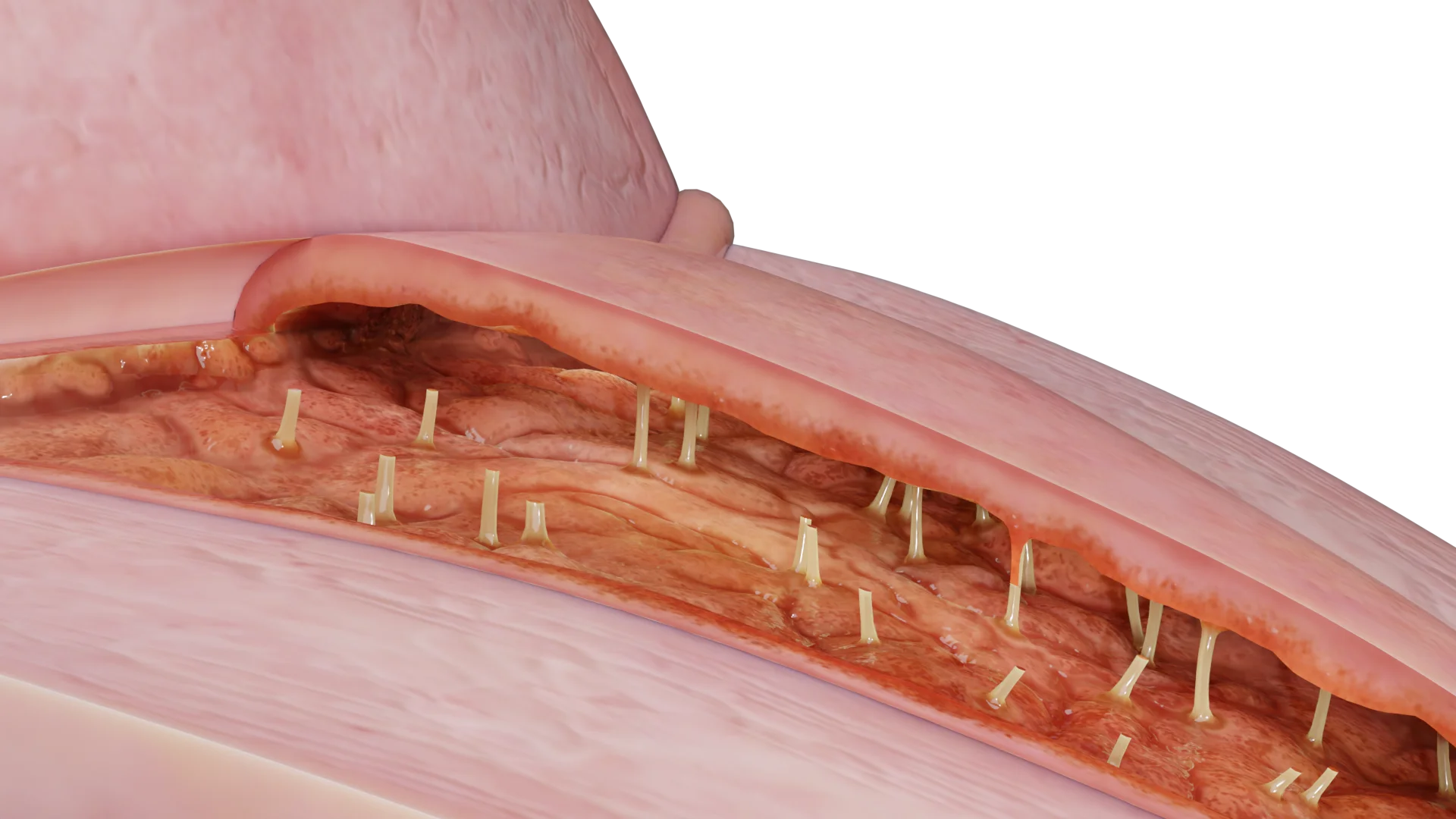
A gynecological speculum examination may reveal a superficial tuberculosis-induced vaginal ulcer with undermined edges. The ulcer bed is infiltrated, and the base is covered with a yellowish or reddish-gray scale. At the edges of the ulcer can be found milky, whitish nodules, which when pressed with a spatula pale. An additional rectal examination is essential to rule out any rectovaginal fistulas.

Tubercular ulcers are a long-term condition. Patients may report general symptoms such as low-grade fever, weakness, decreased energy, fatigue, poor appetite and sleep, night sweats, weight loss, and dry skin.
Histological and cytological examination helps identify specific tuberculous inflammation in obtained samples. A bacteriological or culture test for M. Tuberculosis may use vaginal or ulcer discharge, menstrual blood, or aspirated material as samples. Genital tuberculosis may produce negative bacterial test results, even if the diagnosis has been confirmed microscopically. A nucleic acid amplification test (NAAT) allows for a rapid identification of M. Tuberculosis in samples. Xpert MTB/RIF is a NAAT that helps to both determine and identify the M. Tuberculosis complex. It is also useful in finding any genetic mutations that may indicate rifampicin resistance, one of the most effective tuberculosis medicines. A tuberculin skin test or interferon-gamma release assay (IGRA) is also an option.
Microscopic examination of tissues (biopsy specimens) to detect specific tuberculous granulomas (inflammatory foci containing Pirogov — Langhans cells).
Analyzis of the cellular composition of smears or aspirates to detect signs of tuberculous involvement.
Cultivation of mycobacteria on nutrient media from samples such as vaginal discharge, menstrual blood, ulcer exudates, or biopsy specimens. May give false negative results.
Molecular‑genetic methods (e.g., PCR) for rapid detection of M. Tuberculosis DNA in samples.
An automated NAAT that detects M. Tuberculosis and determines rifampicin resistance by identifying genetic mutations.
Tuberculin is administered to assess the immune response. This is an auxiliary method and cannot be used as the sole means to confirm or exclude tuberculosis.
Blood is tested for levels of interferon-γ produced in response to mycobacterial antigens. An alternative to skin testing.
Combining methods increases diagnostic accuracy, especially when cultures are negative. Histological methods and NAATs (Xpert MTB/RIF) are the most informative.
Find more scientifically accurate content on our social media








The core of therapy for vaginal tuberculosis is long‑term, multidrug anti‑tuberculosis chemotherapy, administered in specialized medical facilities. Treatment is selected individually, taking into account the pathogen’s drug susceptibility, the presence of concomitant diseases, and potential side effects.
Typically, a combination of 3–4 drugs from the following groups is prescribed:
Treatment regimens:
Indicated in cases of:
Treatment must be carried out under close supervision by a phthisiatrician and a gynecologist.
1. What is vaginal tuberculosis?
2. What causes vaginal tuberculosis?
3. What symptoms indicate vaginal tuberculosis?
4. What complications can vaginal tuberculosis cause?
5. How can vaginal tuberculosis be prevented?
6. Can vaginal tuberculosis be completely cured?
7. Is vaginal tuberculosis sexually transmitted?
References
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Tanner MR, Miele P, Carter W, et al. Preexposure Prophylaxis for Prevention of HIV Acquisition Among Adolescents: Clinical Considerations, 2020. MMWR Recomm Rep 2020;69(No. RR-3):1–12.
3.
Aflandhanti PM, Yovi I, Suyanto S, Anggraini D, Rosdiana D. Efficacy of pretomanid-containing regiments for drug-resistant tuberculosis: A systematic review and meta-analysis of clinical trials. Narra J. 2023 Dec;3(3):e402. PMCID: PMC10919689.
4.
WHO consolidated guidelines on tuberculosis: Module 4: Treatment and care [Internet]. Geneva: World Health Organization; 2025. Chapter 2, Drug-resistant TB treatment.
5.
WHO announces landmark changes in treatment of drug-resistant tuberculosis. Geneva: World Health Organization; 2022.
6.
Global Drug Facility [website]. Geneva: Stop TB Partnership; 2023.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io