






Anomalies of Thyroid Gland Development: Classification, Clinical Manifestations, Diagnosis and Treatment

Thyroid developmental anomalies are a heterogeneous group of congenital abnormalities of the thyroid gland due to disruption of embryogenesis.
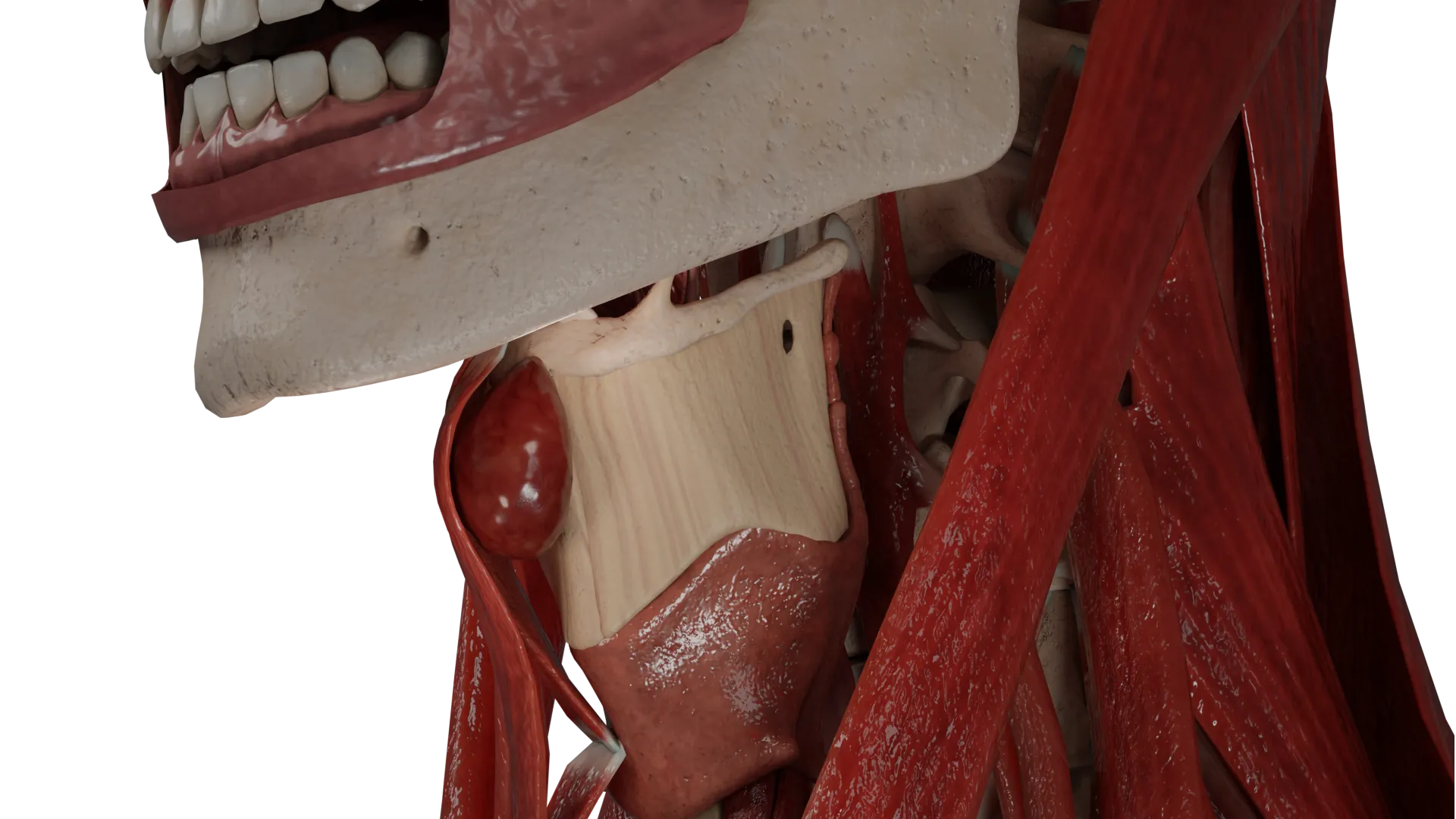
3D models of thyroid developmental anomalies:
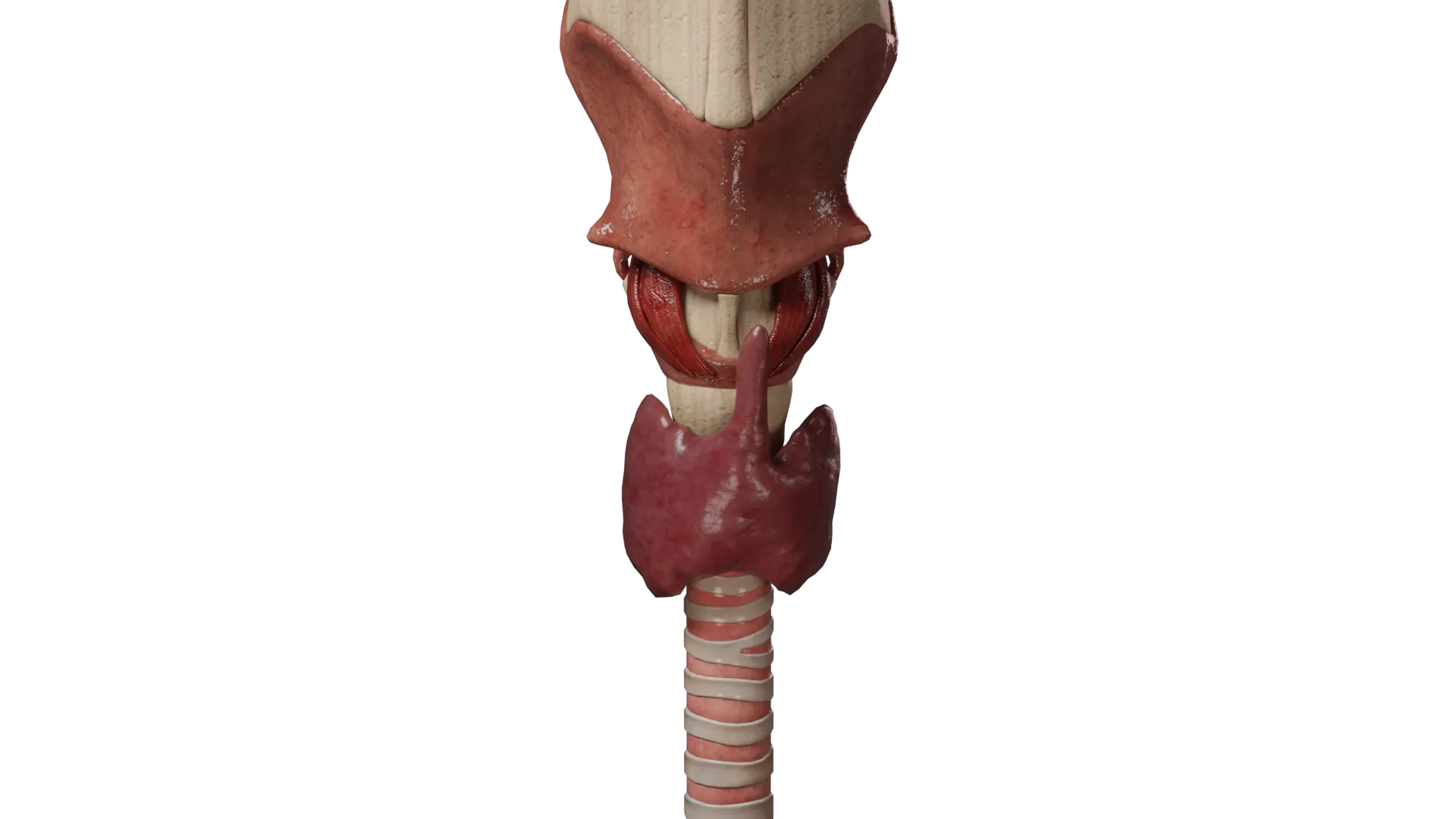
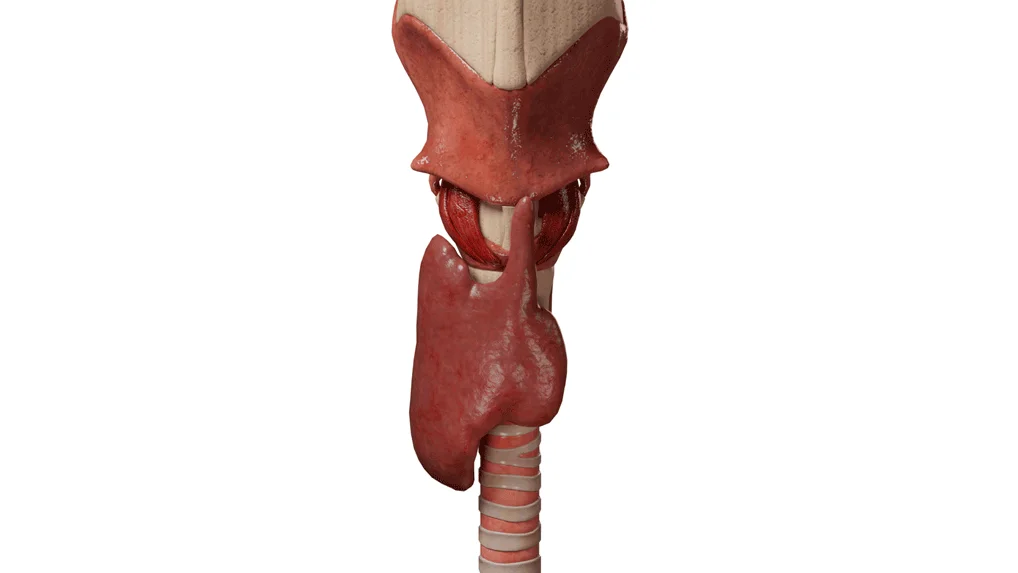 Aplasia of the left lobe of the thyroid gland
Aplasia of the left lobe of the thyroid gland  Lingual ectopia of the thyroid gland
Lingual ectopia of the thyroid gland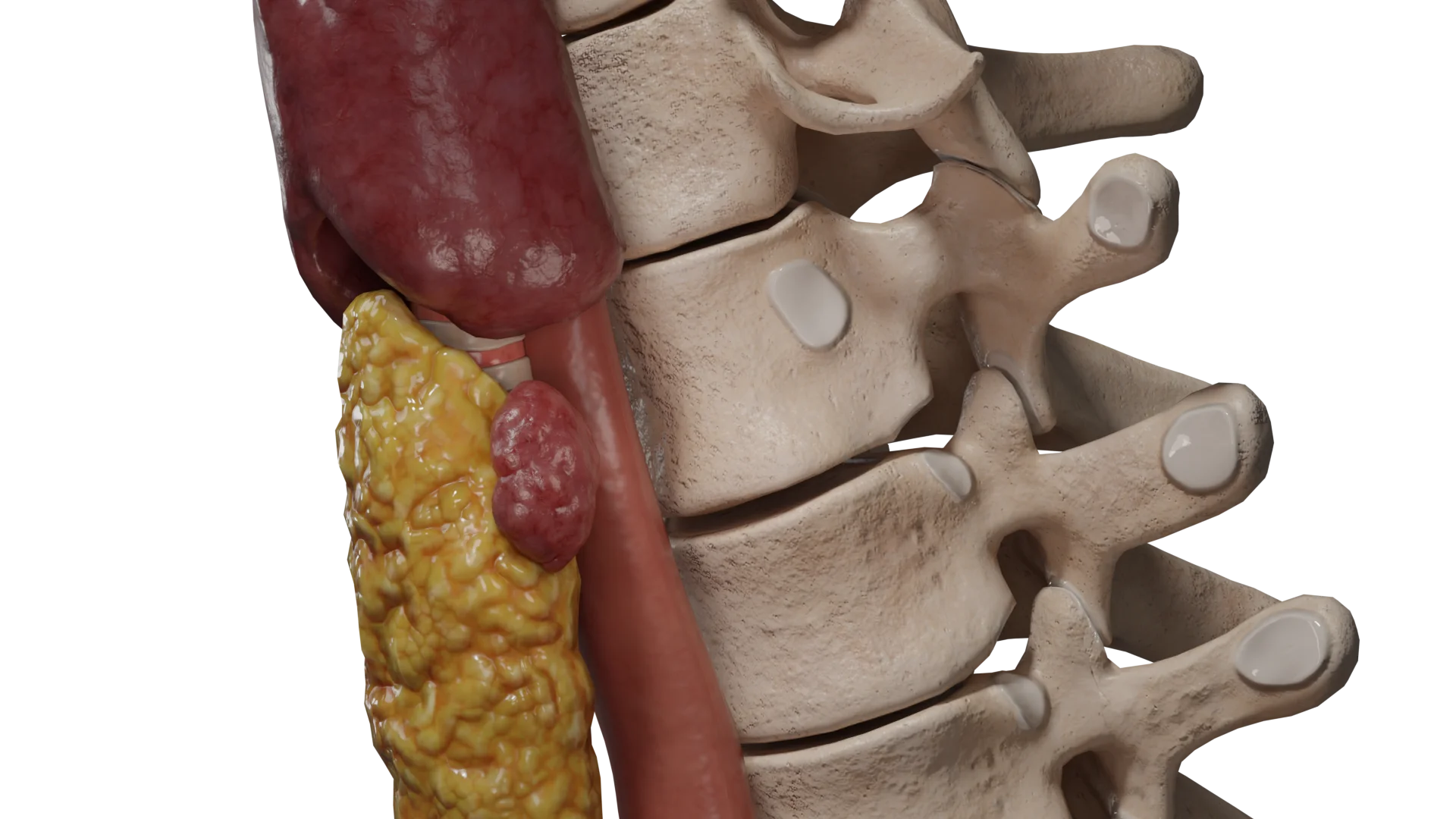 The accessory lobe of the thyroid gland
The accessory lobe of the thyroid glandEmbryology
The thyroid gland in the fetus originates in the 3-4th week of gestation from the entoderm between the first and second gill arches at the base of the tongue and is connected to the pharynx by the thyroid-lingual duct.
From the 5th week of gestation, the process of migration of the thyroid gland begins along the course of the thyroid-lingual duct – from the root of the tongue along the midline caudally to its final position. During migration, the thyroid gland remains connected to the tongue through the thyroid-lingual duct, which closes completely by the 8th week of gestation.
The division of the thyroid gland into right and left lobes occurs in the fifth week of gestation. In addition, in the same week, ultimobranchial cells are formed from the fourth and fifth gill arches, which further differentiate into parafollicular C-cells.
Ultimobranchial cells fuse with the upper dorsolateral part of the developing thyroid gland, forming the tubercle of Zuckerkandl. Parafollicular C cells then spread throughout the thyroid gland, but tend to be located almost entirely in the upper-lateral regions of the thyroid gland.
Developed C cells secrete calcitonin, which lowers serum calcium levels by inhibiting osteoclast function.
Cell differentiation and maturation continue from the 7th to the 12th week of gestation, when the thyroid gland becomes functionally mature and thyroid hormone synthesis begins.
Violation of embryogenesis at any of the above stages leads to the formation of abnormalities of thyroid development.
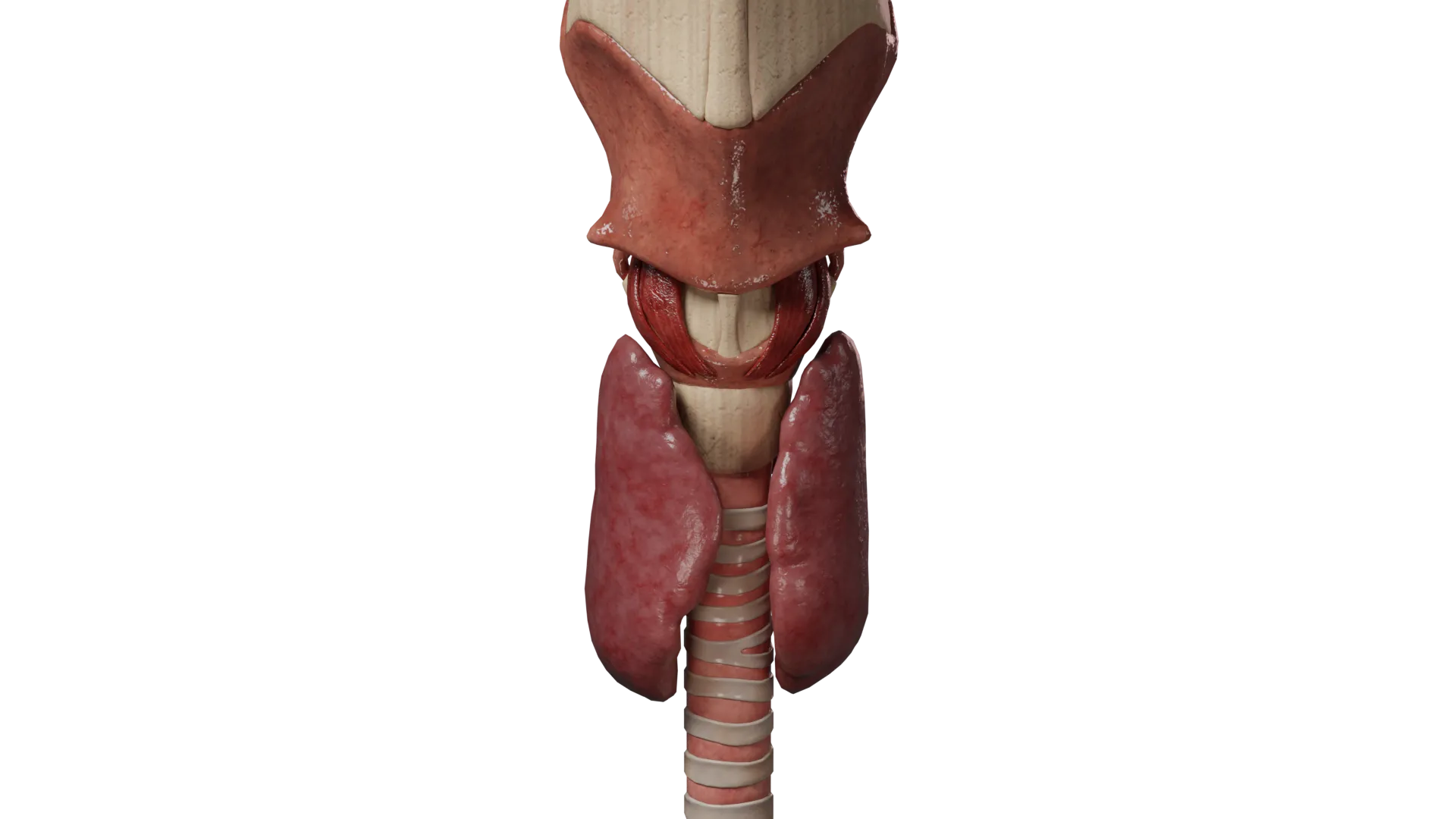
Anatomic Pathology
The thyroid gland is an organ of the endocrine system, which is located on the anterior surface of the neck in front of the trachea at the level of the cervical vertebrae C5-Th1. It consists of right and left lobes connected by an isthmus. From the isthmus, a thin spur called the pyramidal lobe extends upward to the hyoid bone.
The thyroid gland is attached to the trachea by the lateral ligament, or Berry’s ligament. On the posterior surface of each lobe there are pyramidal expansions called Zuckerkandl’s tubercles, the site of fusion of the ultimobranchial bodies with the gland tissue.
Together with the pharynx, esophagus and trachea, the thyroid gland is delimited from the surrounding tissues by the pretracheal fascia.
The thyroid gland is supplied by the right and left superior thyroid arteries (branches of the external carotid arteries) and the right and left inferior thyroid arteries (branches of the thyroid trunk). In 5% of people, the unpaired a. thyroidea ima, which may branch from the brachiocephalic trunk, supraclavicular artery, or aortic arch.
Venous outflow is from the venous plexuses to the right and left superior and middle thyroid veins (flowing into the internal jugular veins), right and left inferior thyroid veins (flowing into the brachial veins).
Lymphatic outflow is to the pre- and paratracheal lymph nodes, then to the jugular lymph nodes and then to the right lymphatic duct and thoracic lymphatic duct.
Innervation:
- The fibers of the sympathetic nervous system emanate from the upper cervical ganglion and form the superior and inferior thyroid nerves;
- Parasympathetic innervation is carried out by branches of the right and left vagus nerve (upper laryngeal and recurrent laryngeal nerves).
Classification of thyroid gland developmental anomalies
- Thyroid dysgenesis:
- Aplasia;
- Hypoplasia;
- Agenesis;
- Ectopia.
- Anomalies of the thyroid-lingual duct:
- Midline cyst of the neck;
- The accessory lobe of the thyroid gland.
Thyroid dysgenesis
Clinical manifestations of thyroid dysgenesis
Thyroid dysgenesis is the most frequent congenital pathology of the endocrine system, its incidence varies from 1:4000 to 1:7000 newborns. According to statistics, up to 85% of cases of congenital hypothyroidism are due to thyroid dysgenesis.
The following risk factors for dysgenesis are distinguished:
- Genetic predisposition: to date, there is a proven relationship between the detection of dysgenesis and the presence of mutations in the TSHR, PAX8, FOXE1, and NKX2-1 genes;
- Intrauterine infections;
- Ionizing radiation during pregnancy;
- Exposure to chemical toxins and pharmacologic agents during pregnancy;
- Iodine deficiency in the diet during pregnancy;
- Autoimmune diseases of the mother during pregnancy accompanied by hypothyroidism.
The following variants of thyroid dysgenesis are distinguished:
- Aplasia – complete absence of the thyroid gland or absence of one (right or left) lobe (this pathology is also called thyroid hemiagenesis.
Aplasia of the thyroid gland is the cause of congenital hypothyroidism.
The typical clinical picture of hypothyroidism in newborns is observed in only 10-15% of cases, which is attributed to the transfer of thyroxine through the bloodstream from the mother. Clinical symptoms develop gradually over a period of 6 weeks, but in severe cases may occur earlier.
Early symptoms of hypothyroidism include:
- Sluggishness;
- Feeding difficulties;
- Large size of the anterior and posterior fontanels;
- Muscle hypotonia;
- Hypothermia;
- Prolonged jaundice;
- A weak or hoarse cry;
- Constipation.
Typical late symptoms include:
- Underdevelopment of the facial bones of the skull, a wide, sunken bridge of the nose (which makes the facial expression frown);
- Swelling of the face, lips, eyelids, wide tongue;
- Bradycardia;
- Muscle hypotonia: bulging abdomen with the presence of umbilical hernia, divergence of rectus abdominis;
- Hyporeflexia;
- Frequent constipation;
- Cold dry leather with a marbled pattern;
- Dry brittle hair, seborrhea of the scalp, forehead, eyelids;
- Respiratory disorders due to edema of respiratory mucosa: stridor, difficult nasal breathing, cyanosis of the nasolabial triangle.
In children after 5-6 months of age, symptoms of delayed psychomotor and mental development come to the forefront. Growth retardation is also noted, which leads to pronounced stunting.
- Hypoplasia is a decrease in the volume and size of the thyroid gland due to underdevelopment of thyroid tissue.
Hypoplasia of the thyroid gland, as well as aplasia, is the cause of congenital hypothyroidism. The severity of thyroid insufficiency symptoms depends on the degree of underdevelopment of thyroid tissue.
- Isthmus agenesis is the absence of the isthmus of the thyroid gland; usually the pyramidal lobe is also absent.
This developmental anomaly is usually asymptomatic and is detected only by ultrasound examination.
- Thyroid ectopia is an atypical location of thyroid tissue. Lingual ectopia is most common, but in rare cases thyroid tissue can occur in both nearby (trachea, larynx, mediastinum) and distant (intestine, ovaries) anatomical structures.
In 7-10% of cases may be asymptomatic and detected only by ultrasound, CT or MRI.
Most cases of thyroid tissue ectopia (up to 70%) lead to the development of hypothyroidism, the severity of clinical manifestations of which is determined by the degree of maturity of thyroid tissue.
About 20% of cases are accompanied by hyperthyroidism. Typical symptoms of thyrotoxicosis include:
- Increased body weight despite reduced appetite;
- Bradycardia;
- Severe weakness and rapid fatigue;
- Drowsiness;
- Swelling of the face and extremities;
- Constipation;
- Dry skin.
In addition to symptoms associated with impaired thyroid hormone production, patients with thyroid ectopia have complaints related to the localization of thyroid tissue in an atypical location.
For example, in lingual ectopia, frequent symptoms may include:
- Sore throat;
- The feeling of a lump in your throat;
- Cough;
- Dysphagia;
- Dysphonia;
- Sleep apnea may develop.
With frequent traumatization, the disease can be complicated by recurrent bleeding, abscessation, and in rare cases (up to 1%) malignization of ectopic gland tissue is possible.
Patients with ectopy of thyroid tissue in the trachea, larynx or mediastinum may complain of breathing difficulties, tachypnea, cyanosis of the skin of the nasolabial triangle. In rare cases, airway obstruction with asphyxia and death may occur.
Diagnosis of thyroid dysgenesis
- Collection of anamnesis, physical examination. Initial examination of the patient reveals characteristic symptoms of hypothyroidism or thyrotoxicosis; laryngoscopy for lingual ectopia allows visualization of thyroid tissue without the use of instrumental diagnostic methods.
- Laboratory diagnostic methods. Determining the level of thyroid hormones in the blood – thyroid hormone (TTH) and thyroxine (sv.T4 and T4) – allows you to assess the function of the thyroid gland, the severity of hypothyroidism or thyrotoxicosis. Additionally, the levels of thyroglobulin (TG), triiodothyronine (T3 and sv.T3), antibodies to thyroperoxidase (ATkTPO), antibodies to thyroid hormone (ATktTG) and antibodies to thyroglobulin (ATktG) are assessed.
- Instrumental visualization techniques:
- Ultrasound (USG) – allows visualization of thyroid tissue. The method is simple, safe, can be used in patients of any age, has high sensitivity and specificity. It is limitedly effective in diagnosing thyroid ectopia.
- Scintigraphy (using radionuclides I123 and Tc99m) is a highly sensitive, highly informative method to assess the localization and functional activity of thyroid tissue. Contraindications for the study are: pregnancy and lactation, individual intolerance to the radiopharmaceutical, severe renal and hepatic insufficiency, fever.
- Computed tomography (CT) or magnetic resonance imaging (MRI).
Treatment of thyroid dysgenesis
Therapy for thyroid dysgenesis includes both medication and surgery.
The asymptomatic course (usually in patients with isthmus agenesis) does not require treatment due to the absence of hormonal abnormalities.
Medical Therapy
- Hormone replacement therapy (HRT)
In aplasia, hypoplasia, ectopia of the thyroid gland, the basis of therapy is the correction of congenital hypothyroidism by means of hormone replacement therapy (HRT) with levothyroxine sodium. It is important to diagnose and start therapy of hypothyroidism as early as possible, because thyroid insufficiency in infants and early childhood leads to irreversible disorders of mental and psychomotor development.
The initial dose of levothyroxine sodium is determined taking into account the estimated needs of the body in thyroxine depending on age:
- In newborns – 10-15 mcg/kg body weight;
- In children – 2-2.5 mcg/kg body weight;
- In adults, 1.5-1.6 mcg/kg body weight.
The thyroxine dose is adjusted according to the thyroid hormone levels in the blood until euthyroidism is achieved.
- Therapy for hyperthyroidism
In thyroid ectopia with the presence of hyperthyroidism, thyrotropic therapy is indicated. Thionamides (thiamazole, propylthiouracil) and glucocorticosteroid hormones are used. The dose of drugs is determined individually based on the severity of thyrotoxicosis. In patients with tachycardia, beta-adrenoblockers are indicated to reduce heart rate (HR) and reduce the risk of arrhythmias.
It is possible to perform radioiodine therapy (RIT) for the treatment of thyrotoxicosis. The feasibility of RIT and the dose of radiopharmaceuticals are determined individually.
Surgical treatment
Surgical treatment of thyroid ectopia is indicated:
- When conservative therapy of thyrotoxicosis is ineffective;
- In the presence of symptoms such as dysphagia, dysphonia, difficulty breathing, compression of other organs by ectopic gland tissue;
- When there is frequent traumatization of tissue with recurrent bleeding or abscessation;
- In the presence of a benign tumor in ectopic tissue and/or if malignancy is suspected.
Total removal of the ectopic thyroid gland within healthy tissues with subsequent hormone replacement therapy with sodium levothyroxine is performed – in cases when the ectopic gland is the only thyroid tissue or in the presence of a normally located thyroid gland with impaired function.
Thyroid-lingual duct anomalies
Clinical manifestations of thyroid-lingual duct anomalies
This group of thyroid developmental anomalies is due to non-enlargement of the thyroid-lingual duct during the embryonic period.
The following variants are distinguished:
- A mid-neck cyst is a non-tumor fluid mass located on the anterior surface of the neck, closely associated with the body of the hyoid bone.
Small cysts have no clinical symptoms. A typical complaint in patients with cysts larger than 5 mm is the presence of an elastic rounded mass in the midline of the neck, movable when swallowing and usually painless.
In 20-60% of cases, the cyst may become infected, which is accompanied by the following symptoms:
- An increase in the size of the cyst;
- Educational morbidity;
- Localized redness of the skin;
- Possible increase in body temperature;
- Possible formation of a fistulous passage on the skin of the anterior surface of the neck.
In rare cases (up to 1-2%) malignization is possible.
- An accessory lobe of the thyroid gland is the presence, along with the normally located thyroid gland, of a separate area of thyroid tissue not associated with the main gland. .
In most cases, the presence of an extra (aberrant) lobe of the thyroid gland is asymptomatic and is detected by routine ultrasound.
If the size of the accessory lobe is large, symptoms of compression of adjacent organs develop:
- The feeling of a lump in your throat;
- Dysphagia;
- Hoarseness of voice;
- Shortness of breath.
It is possible to develop hyperthyroidism due to functional autonomy of the aberrant lobe with typical clinical symptoms.
Diagnosis of thyroid-lingual duct anomalies
The same laboratory and instrumental methods are used in the diagnosis of thyroid-lingual duct anomalies as in the diagnosis of thyroid dysgenesis.
Treatment of thyroid-lingual duct anomalies
Midline cysts of the neck are subject to surgical treatment. Isolated removal of cysts is currently recognized as inappropriate due to the high risk of recurrence (up to 50% according to some authors).
Sistrunk excision is considered the gold standard for surgical treatment of median cysts. The method consists in the removal of not only the cystic cavity, but also resection of the hyoid bone body (to which the cyst closely adjoins), and if the thyroglossal duct is preserved throughout its entire length, excision of the tongue root tissues. The risk of recurrence after removal using the Sistrunk technique is less than 10%.
Asymptomatic aberrant thyroid lobe does not require treatment. In case of symptoms of compression of surrounding organs and/or development of hyperthyroidism due to functional autonomy of the accessory lobe (RFP hyperfixation is determined by scintigraphy with normal or decreased capture by normal gland tissue), surgical treatment is indicated – removal of the aberrant lobe.
FAQ
1. What is hypoplasia of the thyroid gland?
2. What causes can cause thyroid abnormalities?
3. What are the methods for diagnosing thyroid abnormalities?
4. How are thyroid abnormalities treated?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/2.
Mutation of the gene encoding human TTF-2 associated with thyroid agenesis, cleft palate and choanal atresia (R.J. Clifton-Bligh, J.M. Wentworth, P. Heinz, M.S. Crisp, R. John, J.H. Lazarus, M. Ludgate, V.K. Chatterjee).
https://www.ncbi.nlm.nih.gov/books/3.
Anatomy, Head and Neck, Thyroid (Evan Allen; Abbey Fingeret).
https://www.ncbi.nlm.nih.gov/books/4.
Клинические рекомендации «Врожденный гипотиреоз» (Петеркова В А, Безлепкина О Б, Ширяева Т Ю, Вадина Т А, Нагаева Е В, Чикулаева О А, Шредер Е В, Конюхова М Б, Макрецкая Н А, Шестопалова Е А, Митькина В Б).
https://www.ncbi.nlm.nih.gov/5.
Congenital Hypothyroidism (Sasigarn A. Bowden; Marina Goldis).
https://www.ncbi.nlm.nih.gov/books/6.
Thyroglossal Duct Cyst (Janine Amos; Carl Shermetaro).
https://www.ncbi.nlm.nih.gov/books/7.
2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis.
8.
Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement (2014).
