Hypothyroidism: Classification, Clinical Presentation, Diagnosis, and Treatment
Svetlana D.Surgical oncologist, MD
20 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Hypothyroidism is a pathological state characterized by a deficiency of thyroid hormones (triiodothyronine, thyroxine), arising from thyroid gland damage or disturbance in the central regulation of the hypothalamus-pituitary-thyroid axis.
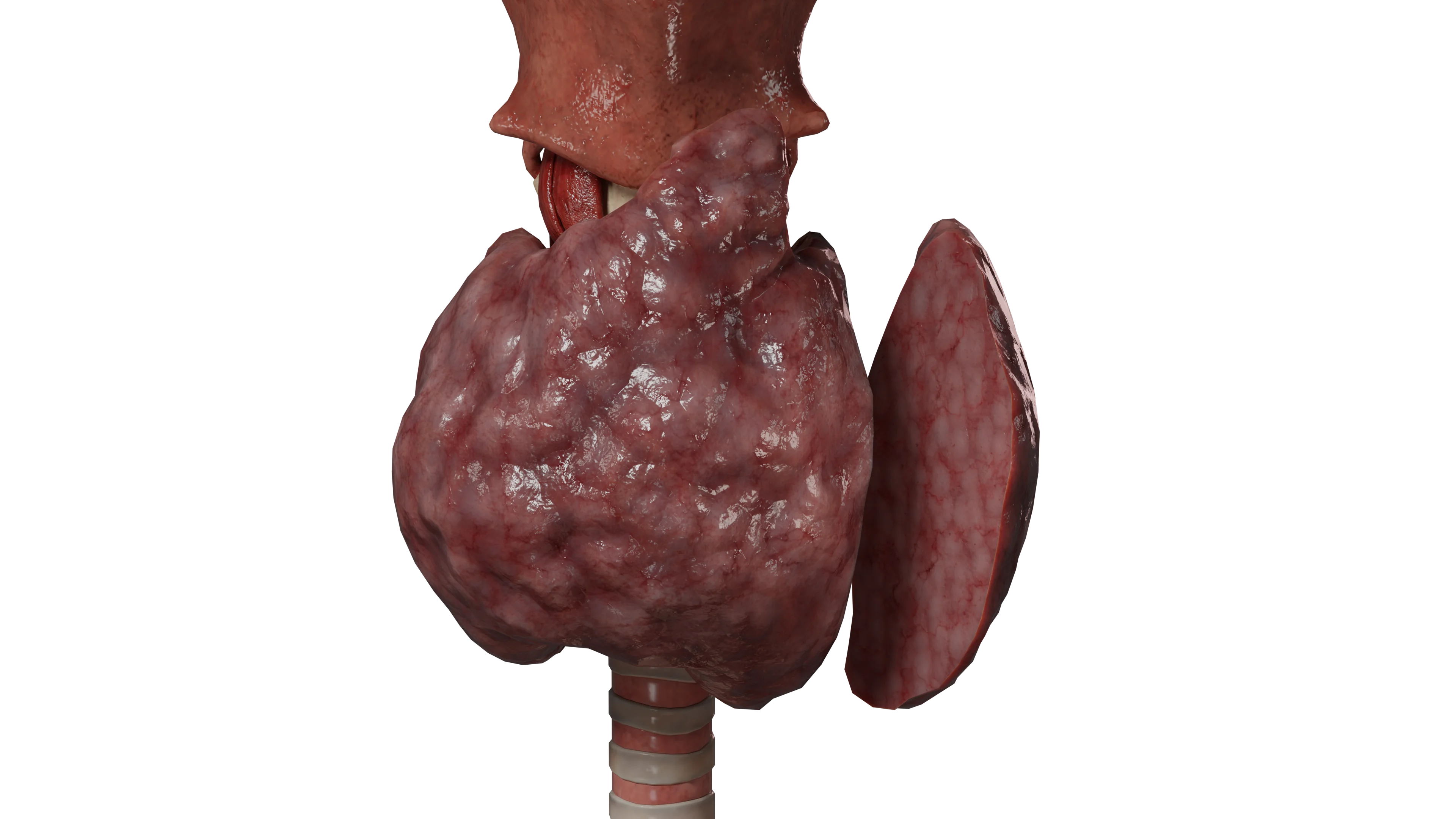
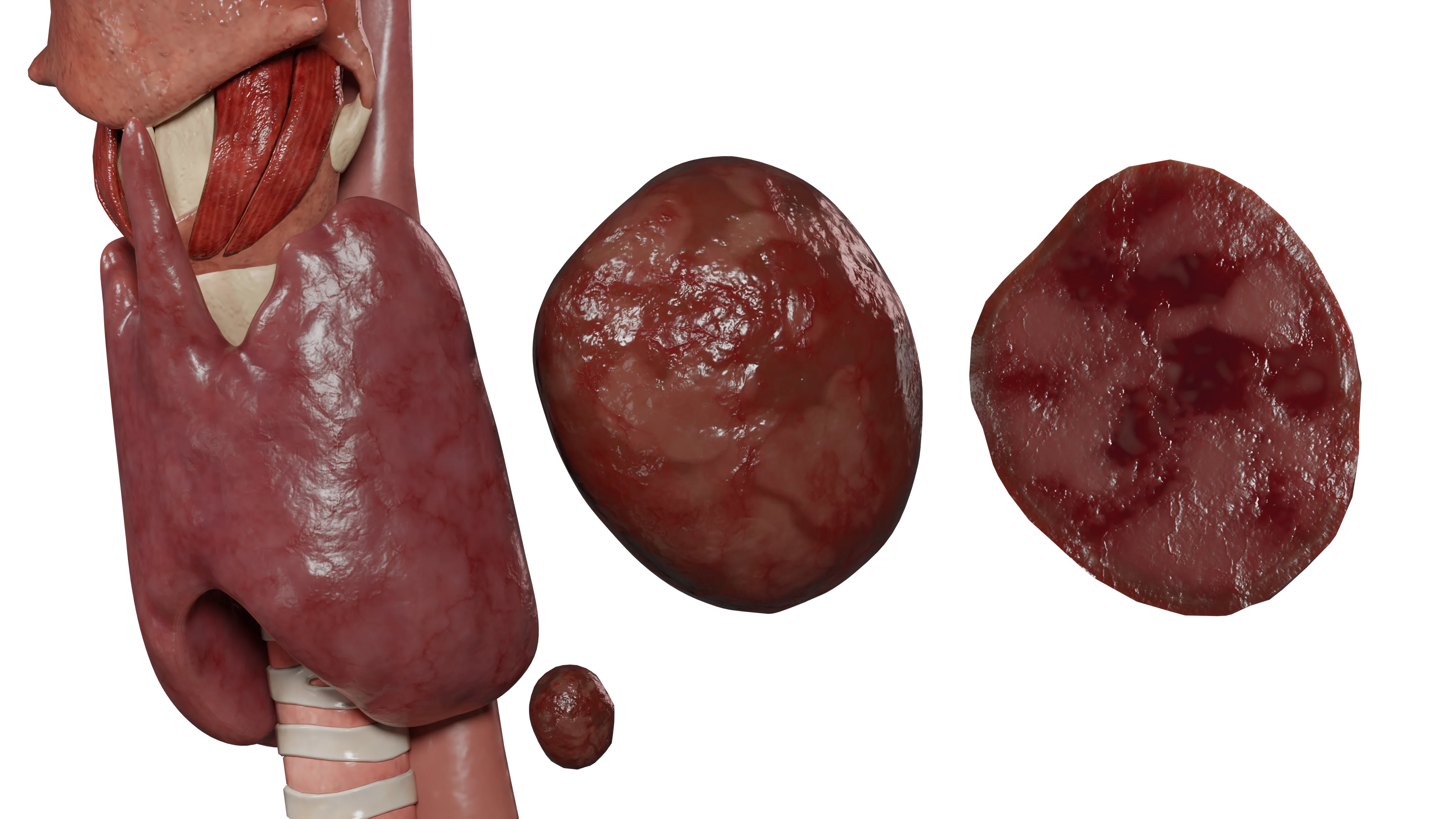
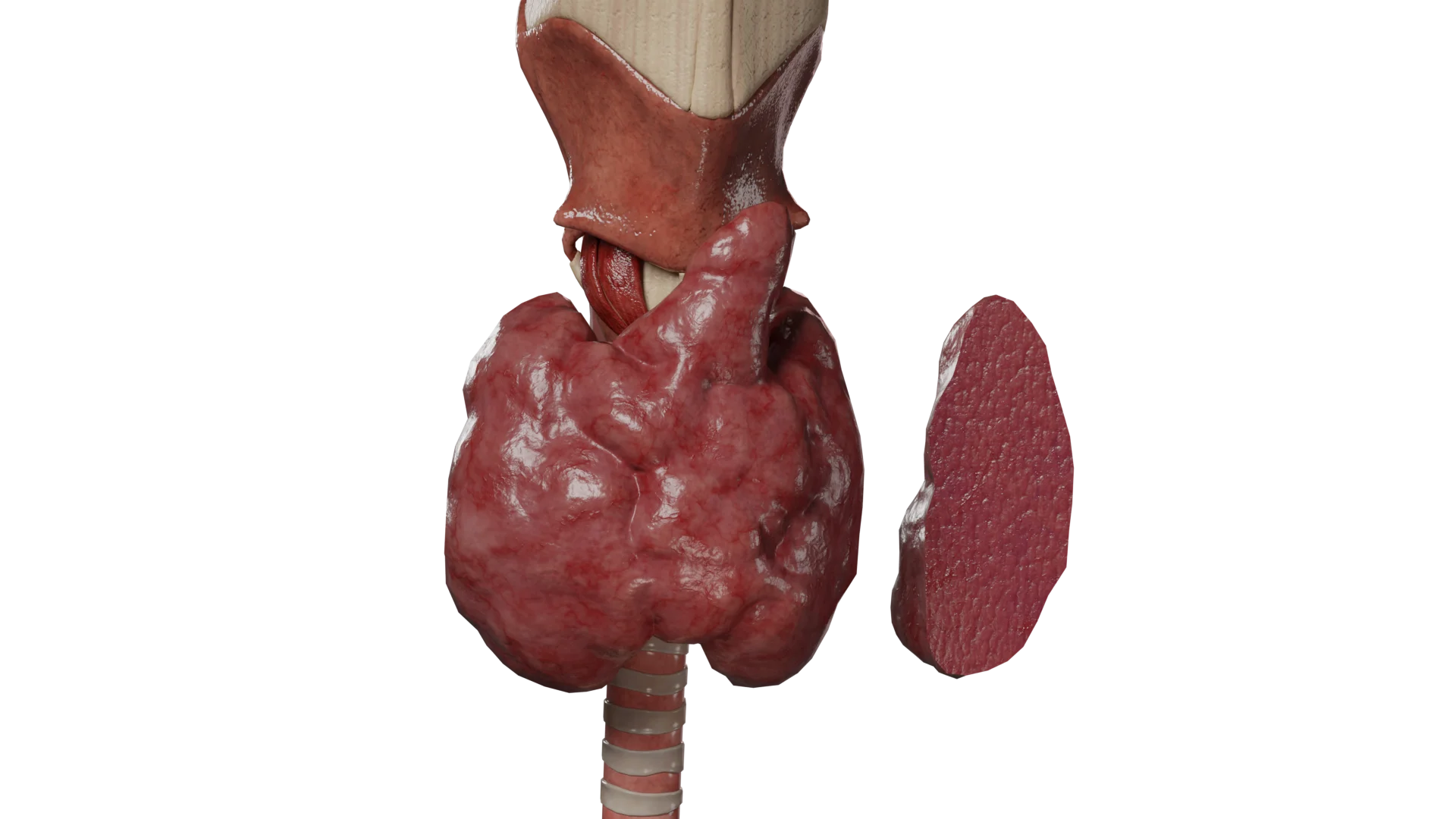
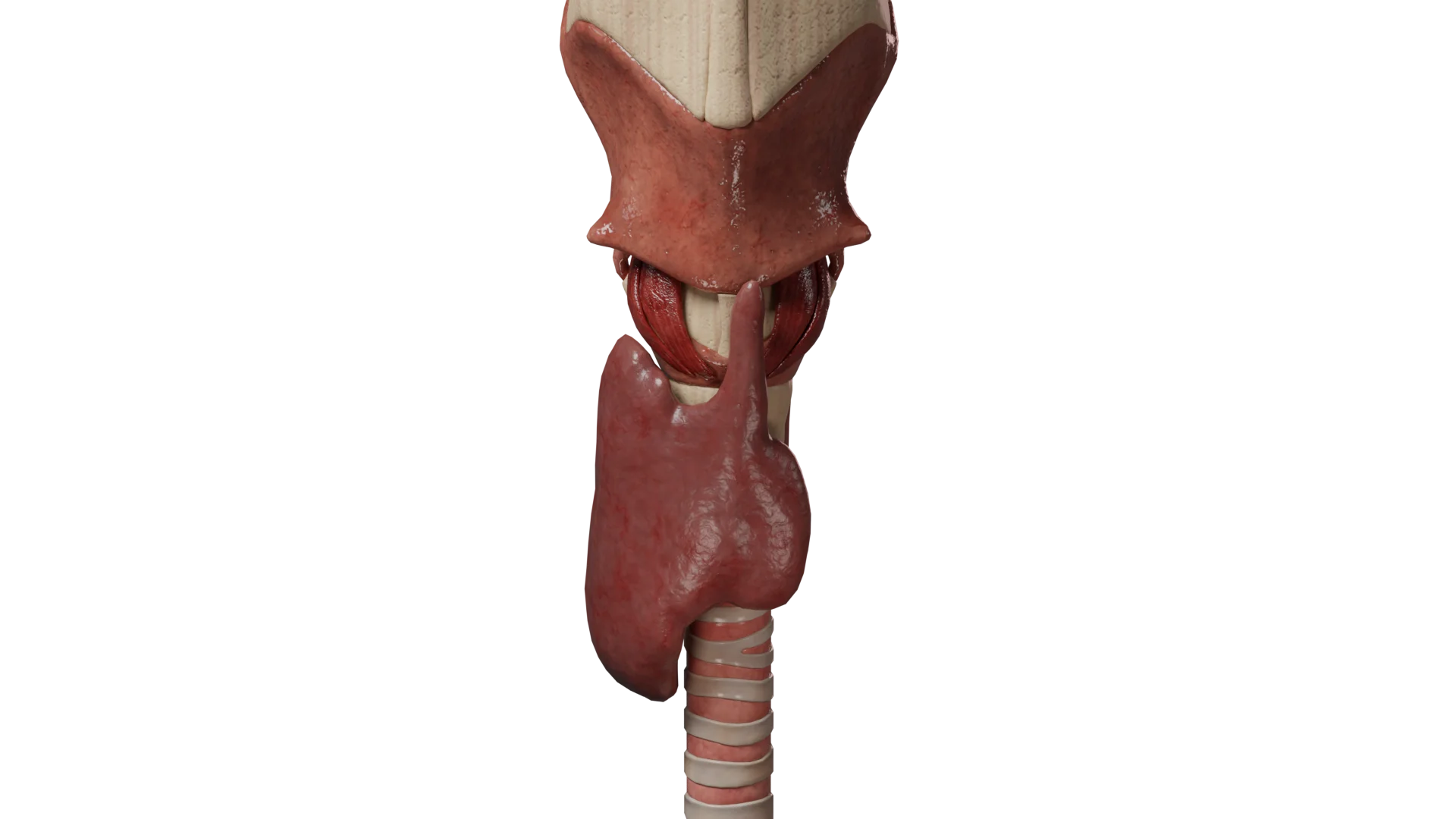
Congenital hypothyroidism: 3D modelAcquired hypothyroidism: 3D model
Classification of hypothyroidism
Hypothyroidism is divided into types based on the level of origin:
Primary hypothyroidism caused by impaired synthesis of triiodothyronine (T3) and thyroxine (T4) by the thyroid gland. It is characterized by decreased levels of T3 and T4 with elevated thyroid-stimulating hormone (TSH) levels;
Secondary hypothyroidism, occurring with decreased synthesis of TSH by the pituitary gland. In secondary hypothyroidism, a deficit of TSH leads to insufficient stimulation of the thyroid gland. This type of hypothyroidism is characterized by decreased levels of TSH, T3, and T4;
Tertiary hypothyroidism, arising from inadequate synthesis of thyrotropin-releasing hormone (TRH) by the hypothalamus, leading to a deficiency of TSH and subsequently T3 and T4.
Depending on the time of manifestation, it is classified as:
Congenital hypothyroidism (detected at birth);
Acquired hypothyroidism (can develop at any age).
Hypothyroidism varies by severity:
Subclinical (latent) hypothyroidism is characterized by increased TSH levels with normal levels of free T4 and T3;
Overt hypothyroidism is characterized by elevated TSH and reduced T4 and T3 levels;
Severe (complicated) hypothyroidism is associated with the development of complications, up to myxedema coma.
Causes of Hypothyroidism
The causes of primary hypothyroidism include the following:
Iodine deficiency in the diet (the most common cause of hypothyroidism worldwide);
Autoimmune diseases of the thyroid gland;
Thyroid dysgenesis;
Use of certain medications;
Thyroid gland surgery;
Previous radiation therapy to the head and neck;
Previous radioiodine therapy.
Causes of secondary hypothyroidism:
Damage to the pituitary gland due to trauma, surgery, radiotherapy, infectious/inflammatory diseases, tumorous lesions, or Sheehan syndrome (postpartum necrosis of the pituitary);
Congenital developmental abnormalities and mutations in genes encoding TSH synthesis.
Causes of tertiary hypothyroidism:
Damage to the hypothalamus due to trauma, surgical or radiological treatment, tumor compression, or inflammatory diseases;
Mutations in genes responsible for TRH synthesis.
Congenital hypothyroidism: causes, clinical presentation, diagnosis, and treatment
Congenital hypothyroidism (CH) is one of the most common preventable causes of intellectual disability, making its early diagnosis and initiation of treatment before the development of irreversible neurological impairments extremely important.
The incidence of CH varies according to different authors from 1:3,000 to 1:4,000 newborns. Differences are observed based on ethnicity: it is higher in Latin American and Asian children (1:1,600 and 1:2,380 cases, respectively), and lower in Black children (1:11,000).
Girls are affected 1.5-2 times more often than boys. The incidence of CH is also higher in multiple pregnancies, older mothers, and premature infants.
Causes of congenital hypothyroidism
The main causes include:
Congenital abnormalities of the thyroid gland, such as ectopia, aplasia, hypoplasia, and agenesis, account for up to 80% of all cases of congenital hypothyroidism;
Defects in thyroid hormone biosynthesis caused by genetic mutations (dyshormonogenesis);
Congenital abnormalities of the pituitary gland and/or hypothalamus (secondary and tertiary hypothyroidism);
Iodine deficiency;
Excessive maternal iodine intake leading to temporary suppression of thyroid hormone synthesis (Wolff-Chaikoff effect);
Transplacental transfer of thioamides taken by the mother during pregnancy;
Transplacental transfer of maternal antibodies blocking the synthesis of thyroid hormones in autoimmune thyroid diseases in the mother (Hashimoto’s thyroiditis).
Symptoms of congenital hypothyroidism
Clinical manifestations of congenital hypothyroidism develop gradually in most cases (more than 80%) within the first 6 weeks of life and are either faintly expressed or not determined at birth. This is due to the transplacental transfer of maternal thyroid hormones to the child (approximately 25-50%).
Early symptoms
The first and earliest symptoms of congenital hypothyroidism include the following:
Large anterior and posterior fontanelles;
Lethargy in infants;
Muscle hypotonia;
Feeding difficulties;
Prolonged jaundice;
Constipation;
Hypothermia;
Weak or hoarse cry.
Late symptoms
In the absence of timely diagnosis and adequate therapy, early symptoms are joined by later ones:
Large broad tongue;
Swelling of the face, eyelids, lips;
Coarse facial features with a sunken nasal bridge due to underdeveloped facial bones;
Coarse, dry, and brittle hair;
Thick, dry, and cold marble-like skin;
Umbilical hernia, abdominal bloating, diastasis recti due to muscle hypotonia;
Hyporeflexia;
Hypotension;
Anemia;
Myxedema with the development of respiratory failure, characterized by noisy breathing, nasal congestion, and periodic perioral cyanosis;
Epiphyseal dysgenesis of the knee joints (delay or disruption in the sequence of ossification center appearance, asymmetry);
Development of myxedema heart disease, a condition caused by interstitial edema, myocardial dystrophy, and intracellular hypokalemia. It manifests with bradycardia, pericardial effusion, and muffled heart tones;
Symptoms of psychomotor and mental retardation, short stature (in children after 5-6 months).
Diagnosis of congenital hypothyroidism
Neonatal screening
Primary
The primary method for diagnosing congenital hypothyroidism is neonatal screening. The method involves determining the level of TSH or T4 from dried blood spots on filter paper collected during the first days of a child’s life.
Test systems used in most countries determine TSH levels due to their simplicity, high sensitivity, specificity, and low cost. Reference values depend on the reagents used and may vary. The method to determine TSH does not allow for the diagnosis of secondary and tertiary hypothyroidism.
Determining T4 levels is a more sensitive method but does not diagnose subclinical forms of hypothyroidism. The ideal but more expensive screening method is the simultaneous determination of both TSH and T4 levels.
Secondary
Secondary screening is carried out in certain categories of newborns, which include:
Premature;
Newborns with low birth weight;
Newborns with the presence of somatic diseases;
Children from multiple pregnancies.
Secondary screening is conducted 2 weeks after the primary one, or in the second week of the child’s life.
Additional diagnostic methods
Thyroid gland ultrasound and scintigraphy allow visualization of dysgenesis (aplasia, hypoplasia, ectopia);
Antibody determination to TSH can be useful in diagnosing transient congenital hypothyroidism caused by maternal autoimmune thyroid diseases;
Serum thyroglobulin determination: a low level or its absence is characteristic of aplasia;
Iodine concentration in urine allows diagnosing of iodine deficiency or excess;
Knee joint X-rays help identify the pathognomonic symptom of congenital hypothyroidism, epiphyseal dysgenesis.
Additional diagnostic methods help clarify the cause of congenital hypothyroidism development but are not decisive in prescribing therapy.
Congenital hypothyroidism treatment
Congenital hypothyroidism treatment involves administering replacement hormone therapy with levothyroxine sodium. Treatment should be started immediately after the diagnosis is made (optimally during the first 2 weeks of the child’s life).
It has been proven that early initiation of therapy and maintenance of normal levels of fT4 allow for normal mental development and prevent severe systemic complications (cardiovascular, respiratory).
According to the Consensus of the European Society for Pediatric Endocrinology, treatment is prescribed based on biochemical criteria:
If TSH in a dry sample is more than 40 mIU/L, therapy is initiated immediately;
If TSH in a dry sample is less than 40 mIU/L, it is possible to delay the start of levothyroxine intake by 24-48 hours until the results of serum TSH and fT4 are obtained;
If the level of fT4 in the blood serum is below the age-appropriate normal value, therapy is initiated immediately, regardless of the TSH level;
If the level of TSH in the blood serum is more than 20 mIU/L, therapy is initiated immediately, regardless of the fT4 level;
If the level of TSH in the blood serum is between 6 and 20 mIU/L and the fT4 level is normal, further examination is indicated to clarify the diagnosis (transient hypothyroidism is possible).
The dose of levothyroxine sodium is determined based on the severity of hypothyroidism.
In severe CH, the medication is prescribed in a dose:
10-15 mcg/kg of body weight per day for full-term newborns;
8-10 mcg/kg of body weight per day for preterm infants in the first 3 months of life;
8-10 mcg/kg of body weight per day at ages 3 to 6 months;
6-8 mcg/kg of body weight per day at ages 6-12 months.
In the case of late initiation of therapy and the presence of heart failure, the initial dose is reduced by 50% and gradually increased to the required level under the control of fT4 in the blood serum every 2 weeks.
TSH and fT4 levels are monitored every two weeks up to their full normalization, then every 1-3 months until 1 year of age. From the age of one to 3 years, monitoring is performed every 2-4 months, and until the completion of growth, every 3-12 months.
Levothyroxine sodium dose adjustment is permissible only under the control of serum TSH and fT4 levels and should aim to maintain their normal age values.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Acquired hypothyroidism: clinical presentation, diagnosis, and treatment
Acquired hypothyroidism is a decrease in thyroid hormone levels, which can develop at any age. It is noted that women are more often affected than men, and the risk of hypothyroidism increases with age.
Clinical symptoms depend on the degree of hypothyroidism severity.
Subclinical form
In subclinical (latent) hypothyroidism, symptoms are usually absent or nonspecific. Patients report complaints:
Increased fatigue;
Impaired memory and concentration;
Somnolence;
Feelings of weakness and chronic fatigue;
Cold intolerance (feeling of chilliness);
Eyelid swelling;
Dry skin;
Hair brittleness;
Weight gain;
Constipation;
Periodic muscle and joint pains;
Menstrual cycle disorders in women.
Overt form
Overt hypothyroidism is characterized by all the above-mentioned symptoms, expressed to a greater extent. Patients progressively develop:
Apathy;
Depression;
Dementia;
Voice changes (hoarseness or roughness);
Severe edema of the eyelids and lower extremities (myxedema);
Menstrual cycle disorders;
Decreased libido;
Infertility.
Severe form
For severe hypothyroidism, in addition to the above symptoms, it is characterized by:
Chronic heart failure;
Severe edema (myxedema) with the formation of effusion in cavities (pleuritis, pericarditis, ascites);
Secondary pituitary adenoma;
Neurological disorders up to the development of myxedema coma.
Myxedema coma
Myxedema coma is an extremely severe, life-threatening condition developed from inadequately selected treatment of severe hypothyroidism or in the untreated cases. In the absence of adequate treatment, mortality reaches up to 80%.
Provoking factors can include:
Severe infectious diseases;
Associated somatic pathology (cardiovascular system diseases, neurological pathology);
Administration of medications such as neuroleptics, beta-blockers, diuretics, barbiturates;
Stress;
Injuries or surgeries.
Symptoms usually develop gradually. This condition is characterized by:
Paleness of the skin;
Hypothermia;
Severe edema of the face and lower extremities;
Hypoglycemia;
Progressively increasing sleepiness;
Apathy;
Confusion;
Development of hallucinations;
Seizures;
Slowing of reflexes up to the development of coma.
Cardiovascular and respiratory system symptoms are characterized by:
Bradycardia;
Arrhythmias;
Hypotension;
Severe dyspnea;
Respiratory depression.
Diagnosis of acquired hypothyroidism
The main method for diagnosing acquired hypothyroidism is laboratory determination of thyroid hormone levels in blood serum (TSH, fT4, and T3).
In addition, the determination of antibodies to thyroid peroxidase (TPO antibodies) is recommended to exclude autoimmune thyroid diseases.
Ultrasound examination of the thyroid gland is used for visualization as a diagnostic refinement method to determine the causes of hypothyroidism and to assess the condition of the thyroid gland.
Treatment of acquired hypothyroidism
Hormone replacement therapy
The primary method of treatment is hormone replacement therapy with sodium levothyroxine.
The recommended initial dose is 1.5 -1.6 mcg/kg body weight for patients under 65 years and without concomitant cardiovascular pathology.
The levothyroxine dose is adjusted individually according to the levels of TSH and free T4 in the blood serum every 4-8 weeks until euthyroid status is achieved.
To minimize the risk of decompensating vascular pathology in patients with cardiac arrhythmias, chronic cardiovascular failure, and those over 65 years of age, levothyroxine therapy is initiated at low doses, calculated individually, with gradual increases under the supervision of the patient’s general condition and serum TSH and T4 levels until euthyroidism is achieved.
After normalization of thyroid hormone levels, the above-mentioned parameters are monitored every 6-12 months.
Treatment of myxedema coma
Treatment of patients is carried out in intensive care and resuscitation units and includes the following methods:
Hormone replacement therapy;
Symptomatic therapy for life-threatening conditions (normalizing body temperature, correcting hypoglycemia, maintaining adequate functioning of the cardiovascular and respiratory systems);
Elimination of factors that provoked the development of the coma.
FAQ
1. How is hypothyroidism different from hyperthyroidism?
The key difference lies in the level of hormone production by the thyroid gland. In hypothyroidism, the function of the organ is reduced, and hormones (T3, T4) are insufficiently produced, slowing down the metabolism. In hyperthyroidism (Graves’ disease), on the contrary, the thyroid gland produces an excess amount of hormones, leading to pathological acceleration of metabolism.
2. What are the risks of hypothyroidism, and what are the consequences if it is not treated?
Prolonged lack of compensation for hormone deficiency leads to systemic disorders, the most dangerous of which are cardiovascular pathologies, including bradycardia, chronic heart failure, and early atherosclerosis. Severe consequences also include secondary immunodeficiency, persistent infertility, deep depression, and cognitive disorders, while in critical situations, a life-threatening complication develops, namely hypothyroid (myxedema) coma, requiring immediate treatment in intensive care and resuscitation.
3. What are the characteristics of hypothyroidism in women and men?
The clinical presentation of the disease in both genders is similar in terms of general metabolic disorders (fatigue, edema, weight gain); however, there are specific gender differences in the reproductive sphere. In women, hypothyroidism often manifests as menstrual cycle disorders, polycystic ovary syndrome, mastopathy, and pregnancy loss. In men, the disease manifests as decreased libido, erectile dysfunction, deterioration in sperm quality, and more evident muscle weakness.
4. Is it possible to treat hypothyroidism without hormones?
Treatment of overt hypothyroidism without hormone replacement therapy is impossible and dangerous. As the disease is caused by a deficiency of vital hormones, the only effective method is external replacement with sodium levothyroxine. Traditional remedies, supplements, or diets cannot restore the lost function of the organ in irreversible changes, and refusing treatment risks severe complications, including coma.
5. How does hypothyroidism affect the nervous system?
Prolonged deficiency of thyroid hormones suppresses the nervous system, often perceived as psychosomatic disorders. Patients complain of apathy, depressive states, memory deterioration, panic attacks, and decreased libido. These manifestations have an organic nature and generally resolve or significantly decrease after normalization of TSH levels against the background of adequate therapy.
6. Is hypothyroidism dangerous during pregnancy?
Yes, uncompensated hypothyroidism during pregnancy is extremely dangerous. Thyroid hormones are critically important for the proper development of the brain and nervous system of the fetus, especially in the first trimester. Lack of treatment can lead to miscarriages, premature births, and intellectual developmental disorders in the child, so strict TSH control and dose correction are necessary for pregnant women.
7. What does a person with hypothyroidism look like?
The appearance of a patient with long-term hypothyroidism has typical features due to myxedema (mucous edema). There is puffiness and swelling of the face, especially the eyelids and lips; the skin becomes pale, dry, and cold. Hair becomes thin, dull, brittle, and falls out excessively; loss of the outer third of the eyebrows is also possible.
8. What diet is needed for hypothyroidism?
There is no special healing diet that can cure hypothyroidism, but nutrition should be balanced with adequate protein, iron, and selenium content. Hypothyroidism slows down metabolism, often leading to weight gain and difficulty losing weight, but after selecting the correct dose of thyroxine, metabolism normalizes and body weight gradually decreases to physiological normal values.
9. Can hypothyroidism resolve on its own?
In most cases, hypothyroidism is a chronic lifelong condition requiring constant therapy, especially if it is caused by autoimmune thyroiditis or gland removal. However, there is transient (temporary) hypothyroidism, for example, postpartum or subacute thyroiditis, which may resolve spontaneously as the function of the thyroid gland is restored.
10. Is there an effective prevention of hypothyroidism?
Primary prevention of the disease is most relevant for endemic iodine-deficient regions and involves adequate iodine intake with food, for example, by using iodized salt. Secondary prevention aims to prevent complications and involves early detection of pathology: individuals in high-risk groups (women over 40 years, positive family history, autoimmune diseases) are recommended to undergo annual TSH level screening.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
J. Jonklaas, A.C. Bianco, A.J. Bauer, K.D. Burman, A.R. Cappola, F.S. Celi, D.S. Cooper, B.W. Kim, R.P. Peeters, M.S. Rosenthal, A.M. Sawka. 2014 Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement.
3.
N. Patil, A. Rehman, C. Anastasopoulou, I. Jialal. Hypothyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK519536/
4.
S.A. Bowden, M. Goldis. Congenital Hypothyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK558913/
5.
A. V. Solntseva. Congenital hypothyroidism in children. Tutorial guide. BGMU 2016 [In Russian].