Hyperthyroidism (Thyrotoxicosis): Symptoms, Causes, Diagnosis and Treatment Methods
Svetlana D.Surgical oncologist, MD
16 min read·December 23, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Hyperthyroidism is a pathological condition due to the hyperproduction of thyroid hormones (thyroxine and triiodothyronine).
Two terms are often used in clinical practice and medical literature and should be distinguished:
Hyperthyroidism is an increase in glandular function (the cause of the condition).
Thyrotoxicosis is a clinical syndrome (symptom complex) resulting from an excess of thyroid hormones in the blood and their toxic effects on body tissues.
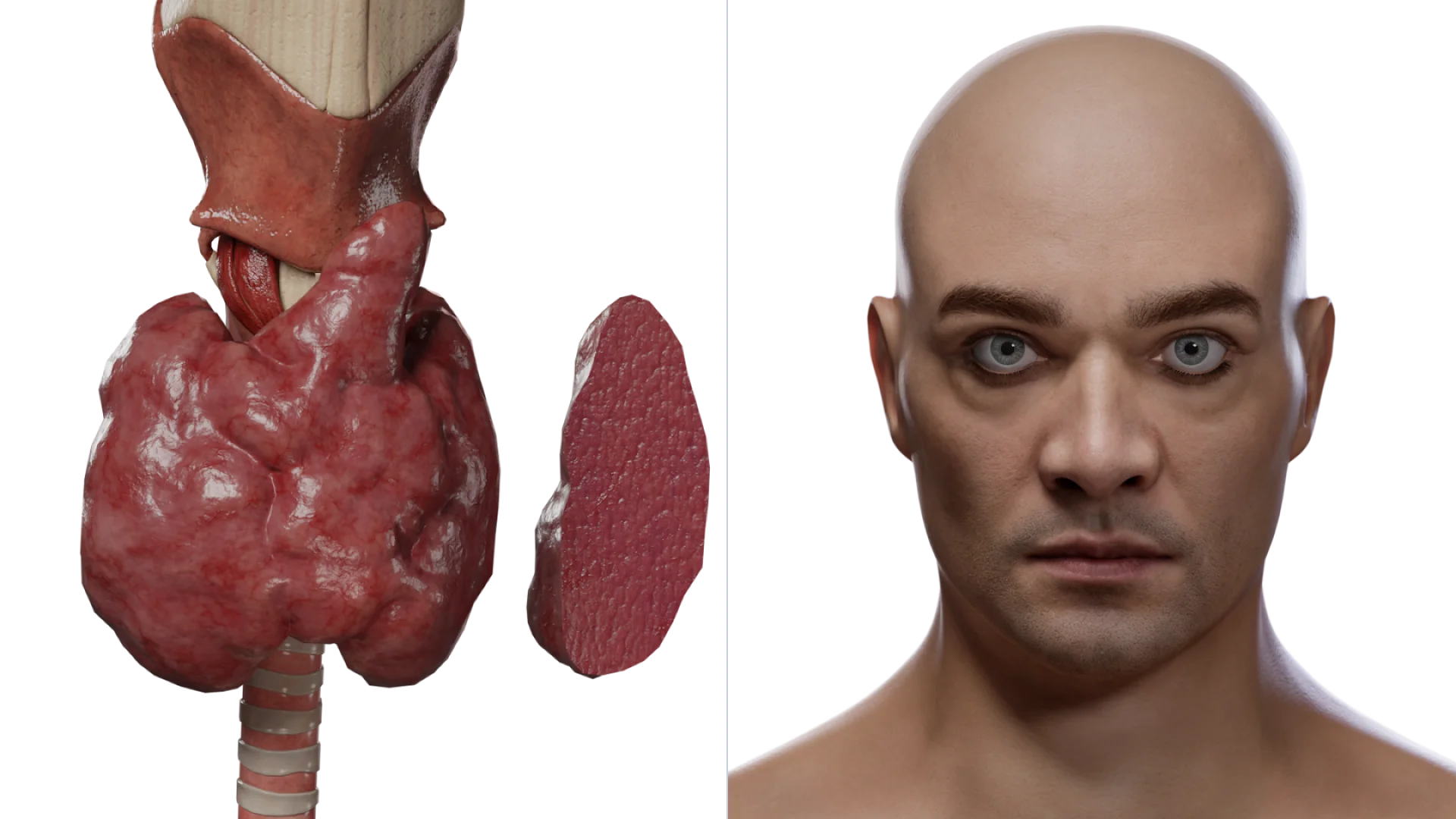
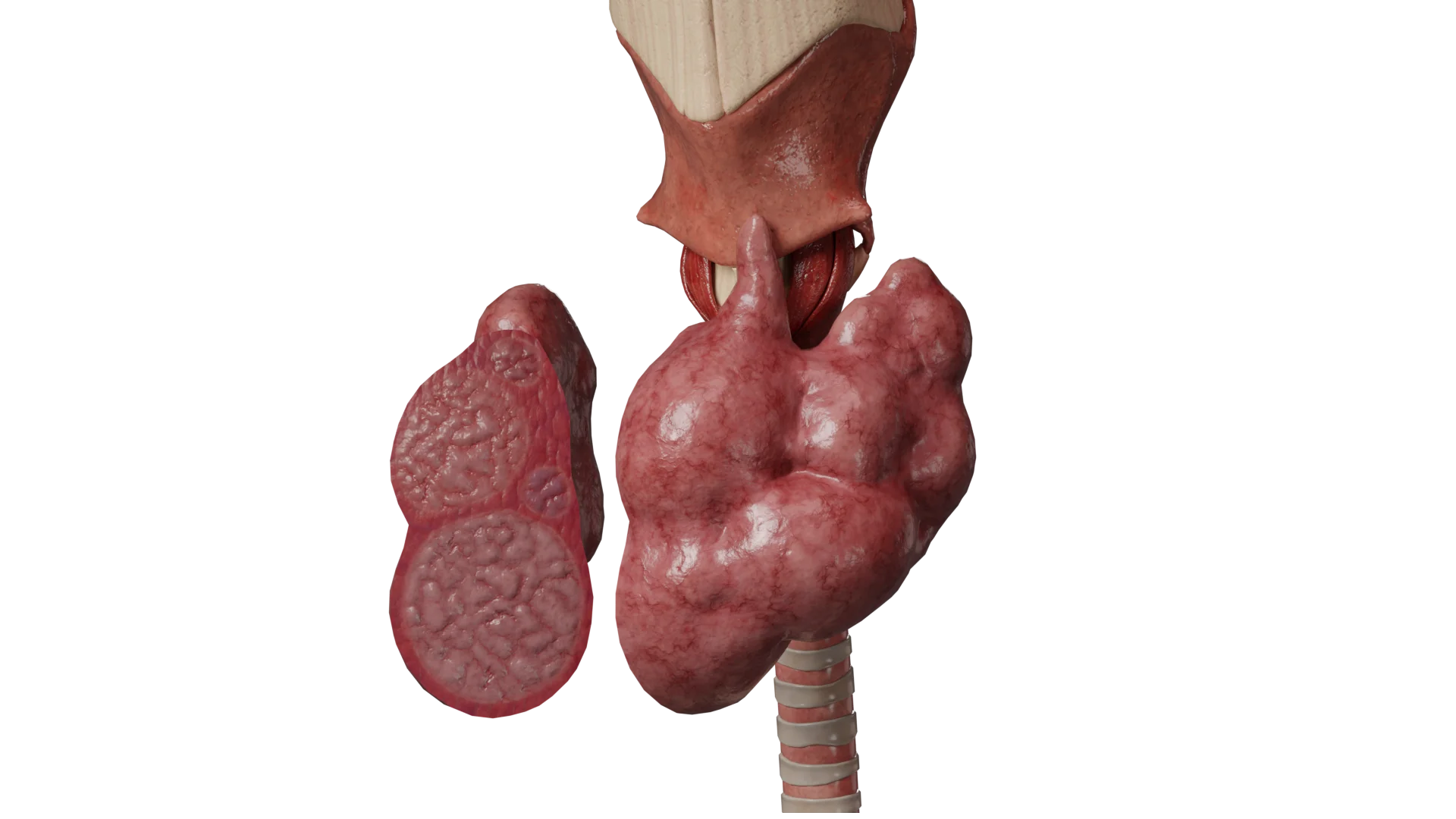
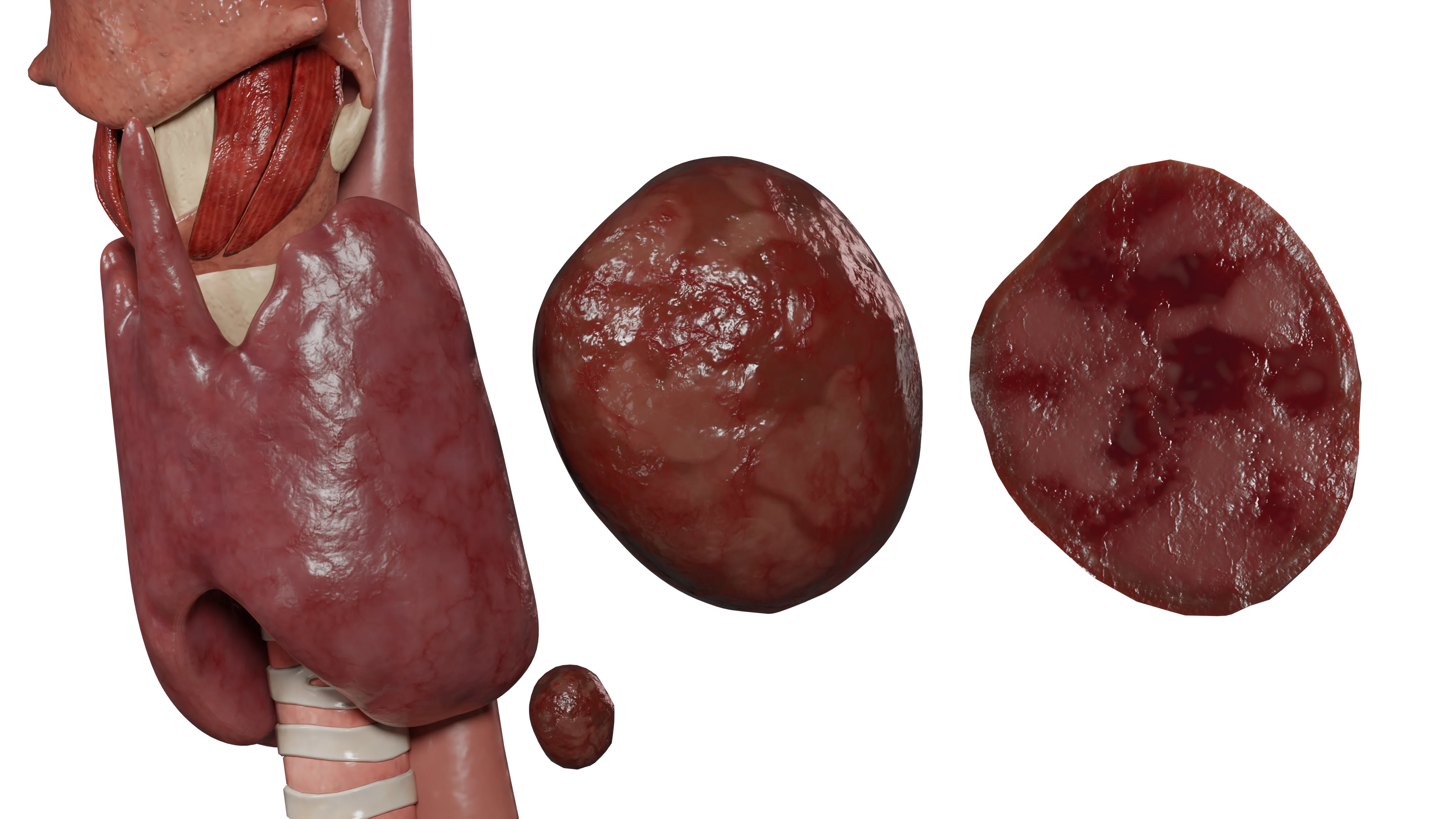
Graves’ disease: cross-sectional view of the thyroid gland (left) and manifestations of the disease (right) – 3D modelMultinodular toxic goiter – 3D model
Classification and types of the condition
Endocrinologists classify pathology by the level of occurrence of the disorder (etiology) and by the severity of clinical manifestations.
Classification by the level of occurrence
Primary hyperthyroidism. It occurs most often. The causes lie directly in the thyroid gland. The main diseases:
Secondary hyperthyroidism. It is a consequence of the hyperproduction of thyroid-stimulating hormone (TSH) by the pituitary gland. It develops in hormonally active tumors (TSH-producing adenomas) or when the pituitary gland resists thyroid hormones.
Tertiary hyperthyroidism. It is caused by a disruption of the synthesis of thyrotropin-releasing hormone in the hypothalamus, which stimulates the secretion of TSH.
Classification of thyrotoxicosis in terms of severity
Clinical classification is based on laboratory values and the severity of symptoms.
Degrees of severity of thyrotoxicosis
Degree
TSH level
T3 and T4 levels
Clinical characterization
Subclinical
Low (below norm)
Within norm
Symptoms are often absent or subtle
Manifest
Low
Elevated
Advanced clinical presentation of thyrotoxicosis
Severe (complicated)
Low
Significantly elevated
In addition to laboratory changes, extrathyroidal symptoms and/or complications develop (atrial fibrillation, heart failure, psychosis, cachexia)
Graves’ Disease is a disease of autoimmune genesis resulting in the hyperfunction of the thyroid gland. It is the most frequent cause of hyperthyroidism. According to various authors, it accounts for up to 60-80% of all cases.
It occurs 7-8 times more often in women than in men. The average age of patients is 20-50 years old, but it can occur in adolescents and the elderly, as well.
Triggers:
Pregnancy and lactation period;
Emotional stress;
Infectious diseases;
Excess iodine in food;
Smoking;
Interferon alpha intake.
Pathogenesis:Thyroid-stimulating immunoglobulin (TSI), also called TSH receptor antibodies (TRAb), plays the primary role. TSI binds to the TSH receptors on the thyrocyte membrane and potentiates the action of thyroid hormone. This leads to both increased thyroid hormone synthesis (hyperthyroidism) and glandular hyperplasia (overgrowth).
Plummer’s Disease is the second-most common cause of thyrotoxicosis. It usually develops in individuals over the age of 50 years and more often in women.
Plummer’s Disease develops from a long-standing, non-toxic multinodular goiter when one or more nodes acquire functional autonomy. They begin to produce hormones uncontrollably, suppressing the function of healthy tissue and lowering TSH levels.
Toxic adenoma is a benign thyroid neoplasm (usually solitary) with functional autonomy due to somatic mutations in the gene encoding thyroid-stimulating hormone receptor (TSHR).
Excessive thyroid hormone production by the tumor leads to the development of hyperthyroidism and suppresses normal thyroid tissue function.
The clinical presentation consists of typical symptoms of thyrotoxicosis, as well as a single thyroid nodule that is palpably identifiable and, for large tumors, visually identifiable.
Diagnosis of the disease includes collecting anamnesis, physical examination of the patient, laboratory test (determination of TSH & T4 levels in serum), and instrumental methods of investigation. Ultrasonic diagnostics and scintigraphy are used to visualize the formation. The latter makes it possible to reliably assess the tumor’s functional autonomy, which plays a decisive role in forming a diagnosis.
Toxic thyroid adenoma is treated via surgical removal via hemithyroidectomy or resection of the thyroid lobe in which the tumor is present.
Medication- or drug-induced thyrotoxicosis is an endocrine pathology in which hyperproduction of thyroid hormones is caused by taking certain medications.
The prevalence of drug-induced hyperthyroidism is not reliably known. According to different authors, it ranges from 1.4% to 64% when taking amiodarone, from 14.8% to 33% when taking alemtuzumab, and up to 1.7% with lithium drugs.
Drug-induced hyperthyroidism can develop against the background of taking the following drugs:
Overdose of thyroxine or iodine preparations;
Amiodarone;
Alemtuzumab;
Tyrosine kinase inhibitors;
Interferons;
Lithium preparations;
Prostaglandins.
The mechanisms for the development of drug-induced thyrotoxicosis may vary by drug, but the basis is usually autoimmune disorders and toxic damage to thyrocytes.
Risk factors for the development of drug-induced thyrotoxicosis include:
Concomitant thyroid pathology (e.g., chronic autoimmune thyroiditis) when starting to take hyperthyroidism-inducing medications;
A history of thyroid disease (e.g., postpartum thyroiditis);
An aggravated family history of thyroid disease;
Female sex.
The clinical presentation is identical to other forms of hyperthyroidism, but the development of symptoms is associated with the intake of certain drugs.
When diagnosing drug-induced thyrotoxicosis, the key role is played by anamnestic data, namely the fact of taking drugs that induce the development of hyperthyroidism, as well as laboratory and instrumental methods of research.
The main methods of treatment:
Cessation of medications that provoked the development of thyrotoxicosis (if possible);
Medication thyreostatic and symptomatic (beta blockers) therapy;
Surgical treatment via thyroidectomy if non-surgical therapy has no effect.
Clinical Manifestations and Symptoms
Regardless of the cause for the increase in hormone levels, the general symptom complex of thyrotoxicosis develops:
Nervous system: emotional lability (anxiety, excessive excitability, tearfulness), fine tremor of fingers of outstretched hands, and sleep disorders.
Metabolism: progressive weight loss (while appetite is preserved or even increased), muscle weakness, and rapid fatigue.
Thermoregulation: increased sweating, heat intolerance, constantly moist and hot skin, and subfebrile temperature.
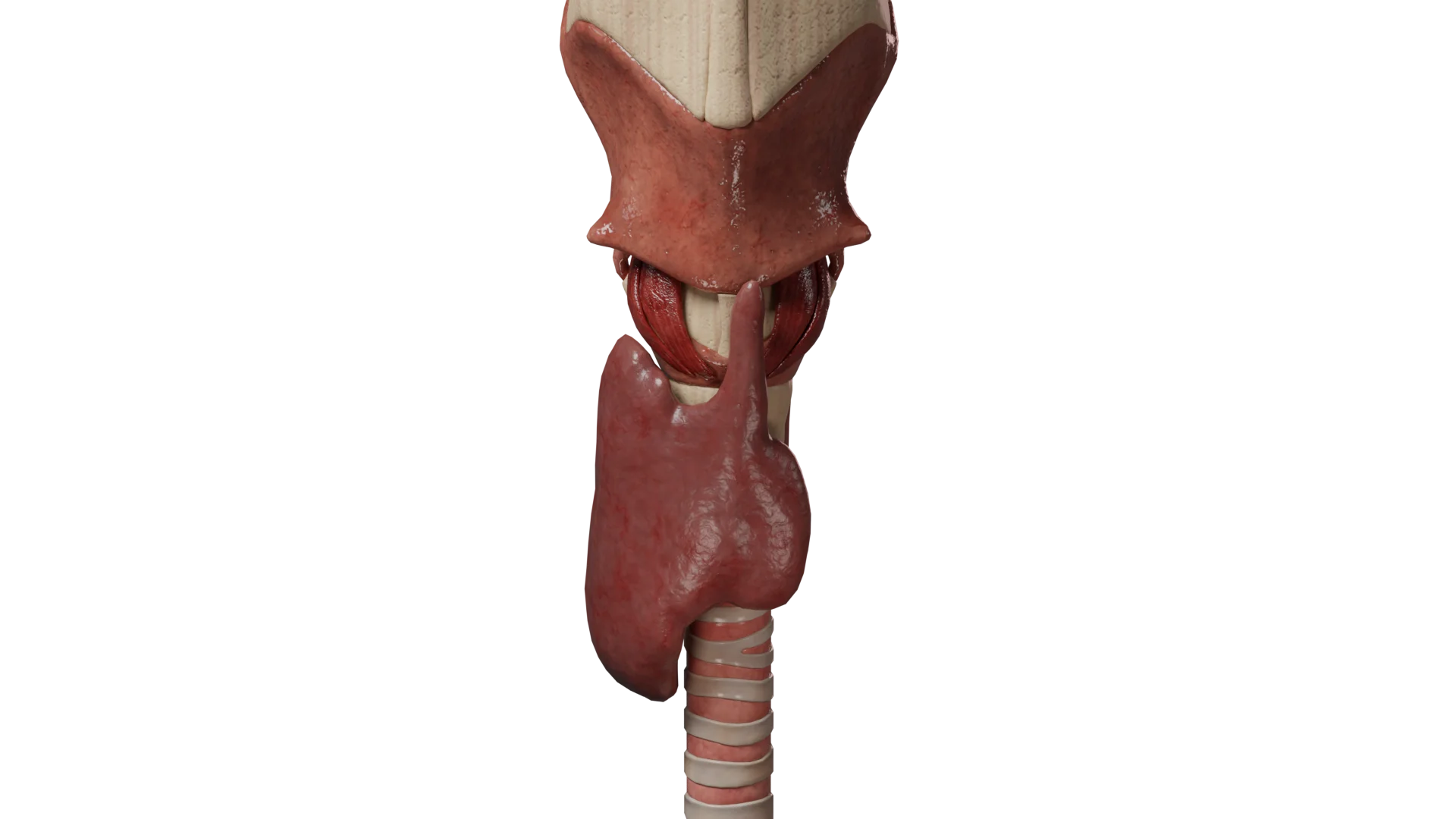
Local changes: diffuse or nodular enlargement of the thyroid gland (goiter).
Specific symptoms of Graves’ Disease
In addition to the general signs of thyrotoxicosis, the presence of extrathyroidal lesions is characteristic:
Endocrine ophthalmopathy (EOP), also known as Thyroid Eye Disease (TED). It occurs in 30% of cases. It’s associated with autoimmune inflammation of the retrobulbar fibers. Manifestations: lacrimation, photophobia, eye grittiness, and periorbital edema. If it progresses, it leads to exophthalmos, lagophthalmos, and diplopia.
Pretibial myxedema (thyroid dermopathy). It occurs in 2-3% of cases. It is manifested by swelling and thickening of the skin of the lower leg (similar to an orange peel), localized mainly on the anterior surface.
Thyroid acropachia. It occurs in approximately 1% of cases. The distal phalanges of the fingers and toes thicken, and soft tissue edema and periosteal reactions occur.
Other forms of clinical presentation
Multinodular toxic goiter: symptoms gradually increase. Extrathyroidal symptoms (ophthalmopathy, myxedema) are absent. Exophthalmos is rare. Upon palpation, individual nodes are detected, and the gland is lumpy.
Toxic adenoma: the clinical presentation consists of typical symptoms of thyrotoxicosis, as well as a single thyroid nodule that is palpably identifiable and, for large tumors, visually identifiable.
Diagnosis of hyperthyroidism
The diagnostic method includes:
Collecting history and conducting an examination. Evaluating complaints, tremors, and ocular symptoms, as well as palpating the neck. For drug-induced thyrotoxicosis, taking drugs that induce hyperthyroidism plays a key role.
Laboratory tests:
TSH: primary marker. It is low in primary hyperthyroidism.
T3 and T4: if TSH is decreased, levels of the free fractions of hormones are determined. In subclinical thyrotoxicosis, they are normal; in manifest thyrotoxicosis, they are elevated.
TSH receptor antibodies (TRAb): used for differential diagnosis. In Graves’ Disease, the index is elevated; in other forms, it is often normal.
Blood chemistry: possible hypocholesterolemia, increased hepatic transaminases, alkaline phosphatase, and hypercalcemia.
Total blood count: possible microcytic anemia, thrombocytopenia.
Thyroid ultrasound. This is the main method of visualization, and it makes it possible to assess the volume, echogenicity, and presence of nodules.
Scintigraphy (with I-123 or Tc-99m). Assesses function and makes it possible to detect ‘hot’ nodules (in Plummer’s Disease and toxic adenoma) or diffuse entrapment (in Graves’ Disease). This is a crucial method for confirming the functional autonomy of the adenoma.
Orbital CT/MRI. This is a clarifying method in ophthalmopathy.
Methods of treatment of hyperthyroidism
The choice of method depends on the cause, severity of thyrotoxicosis, and concomitant pathology.
1. Drug therapy (Thyreostatics)
Administration of thionamides can achieve remission in 35% to 50% of patients with Graves’ Disease.
Initial therapy: administered with maximal doses (30-40 mg/day of thiamazole in 2-3 doses or 300 mg/day of propylthiouracil in 3-4 doses).
Maintenance therapy: after normalization of T4 (usually after 4-6 weeks), the dose is gradually reduced to maintenance (2.5-10 mg/day for thiamazole and 12.5-50 mg/day for propylthiouracil).
Duration: the course of treatment is 12-24 months.
Side effects: allergies, arthralgias, toxic hepatitis, and agranulocytosis (critical decrease in white blood cells).
Symptomatic therapy: patients with a HR of > 90 beats/min, as well as the elderly, are prescribed beta blockers (up to 100 mg/day of atenolol, 5-10 mg/day of bisoprolol, and up to 40 mg/day propranolol). If contraindications to them (asthma) occur, calcium channel blockers (verapamil or diltiazem) can be used. In severe thyrotoxicosis and adrenal insufficiency, glucocorticosteroids are indicated.
2. Radioiodine therapy (RIT)
The use of radioactive iodine I-131 to destroy thyrocytes.
Indications: ineffectiveness or intolerance of thyrostatics, relapse of the disease, and contraindications to surgery.
Contraindications: pregnancy, lactation, severe ophthalmopathy, large thyroid volume, and the presence of nodal pathology in the gland.
Course: thyreostatics are discontinued 5-7 days before isotope administration. The dose is calculated individually or is fixed (10-25 mCi).
Results: hypothyroidism develops after 6-12 months (requires prescription of L-thyroxine).
3. Surgical treatment (Thyroidectomy).
Radical method: removal of the thyroid gland.
Indications:
Gland volume >35-40 ml with compression phenomena.
Severe course of thyrotoxicosis and lack of remission after 2 years of therapy.
Intolerance to thyrostatics.
Suspicion of oncology.
Multinodular toxic goiter and toxic adenoma (method of choice).
Preoperative preparation: mandatory achievement of euthyroidism by medication to prevent thyrotoxic crisis.
Post-surgery: lifelong hormone replacement therapy with levothyroxine sodium (1.5-1.6 mcg/kg body weight per day). TSH monitoring every 6-8 weeks until dose adjustment.
Surgical complications: bleeding, septic complications, hypoparathyroidism, and laryngeal paresis or paralysis.
Treatment of endocrine ophthalmopathy
Mild form: symptomatic therapy (hydration, glasses), normalization of hormones.
Severe form: pulse therapy with glucocorticosteroids (methylprednisolone start 500 mg/week, prednisolone orally 100 mg/day with reduction). If ineffective, the next method is monoclonal antibodies (teprotumumab, rituximab) or surgical decompression of the orbit.
Features of treating individual forms
Drug-induced thyrotoxicosis: withdrawal of the provocateur drug, thyrostatics, and symptomatic therapy. In the absence of effect, thyroidectomy.
Endocrine ophthalmopathy: in the mild form, symptomatic therapy. In severe forms, pulse therapy with glucocorticosteroids, monoclonal antibodies (teprotumumab), or surgical decompression of the orbit.
Complications of thyrotoxicosis
A prolonged course of thyrotoxicosis without adequate treatment leads to systemic damage to the body. Thyroid hormones in excess act as a “toxin” to vital organs.
Major complications include:
Thyrotoxic myocardiodystrophy, in which excess hormones have a direct toxic effect on the heart muscle. This leads to the depletion of myocardial energy reserves, enlargement of heart cavities, and congestive heart failure (edema, dyspnea, intolerance to exertion).
Atrial fibrillation which is one of the most frequent complications. It is characterized by chaotic atrial contraction, which significantly increases the risk of thrombosis and ischemic stroke.
Toxic hepatitis, which is liver damage caused by metabolic disorders amid excess hormones. It is characterized by jaundice of the skin and sclerae, as well as an increase in liver enzymes (ALT, AST).
Osteoporosis, in which thyroid hormones stimulate the destruction of bone tissue and calcium leaching. Bones become brittle, and fractures occur even with minor injuries (secondary osteoporosis).
Reproductive disorders, in which women can develop dysmenorrhea (cycle failures) up to amenorrhea and infertility. Men experience decreased libido, erectile dysfunction, and gynecomastia.
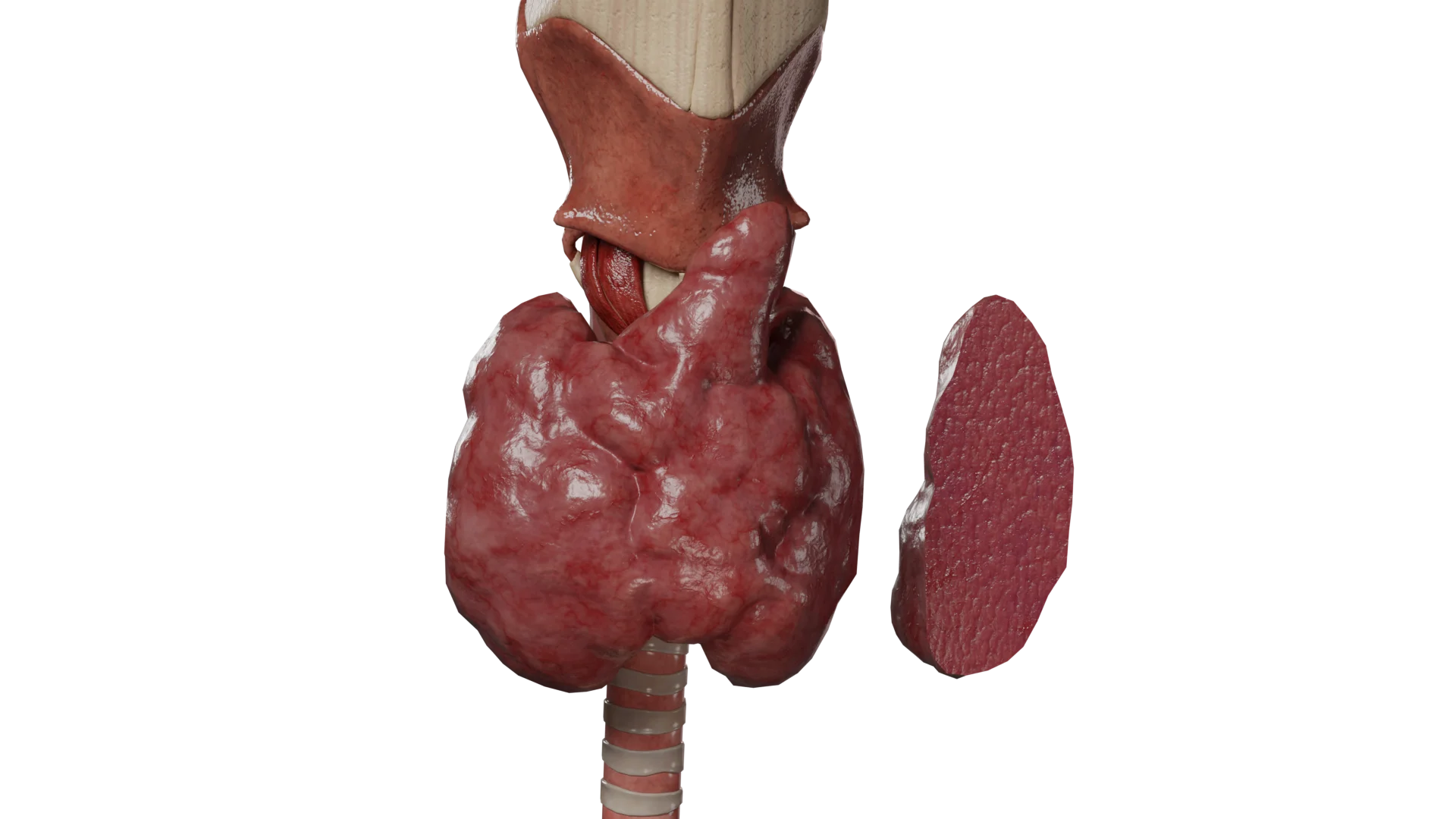
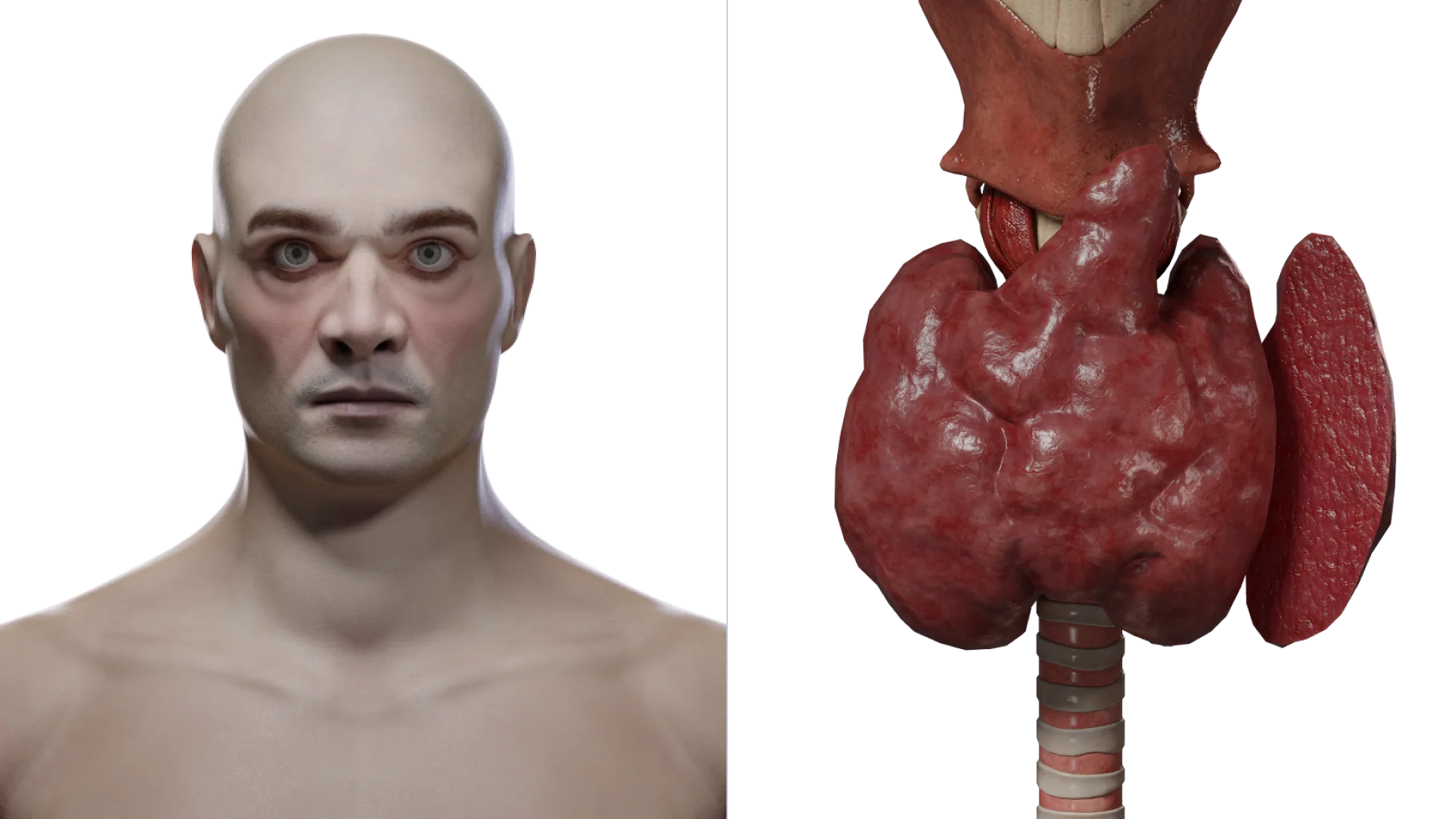
Thyroid storm
Thyroid storm: manifestations of the disease (left) and cross-sectional view of a thyroid gland (right) – 3D model
A rare, life-threatening complication, with a mortality rate of up to 60%.
Causes: the abrupt release of large amounts of thyroid hormones after thyroidectomy in the absence of adequate preoperative preparation (decompensated thyrotoxicosis); excessive physical and emotional stress; pregnancy and lactation; severe infectious diseases.
Symptoms:
Fever of up to 40-41°C.
Tachycardia >150 beats/min, arrhythmia, and acute heart failure.
Psychomotor agitation, psychosis progressing to coma.
Vomiting, diarrhea, and jaundice.
Adrenal insufficiency.
Treatment: infusion, thyrostatic therapy, administration of glucocorticosteroid hormones, and symptomatic therapy. If drug therapy is ineffective, plasmapheresis or hemoperfusion is indicated.
FAQ
1. What is hyperthyroidism in simple words?
This is a condition in which the thyroid gland works too actively and produces an excess of hormones, which “accelerates” the metabolism and leads to wear and tear on the body.
2. What is the difference between hyperthyroidism and hypothyroidism?
These are opposite conditions. In hyperthyroidism, there are too many hormones (the metabolism is accelerated), and in hypothyroidism, there are too few (the metabolism is slowed).
3. Can hyperthyroidism be completely cured?
Surgical treatment (thyroidectomy) completely removes the cause of excess hormones but leads to hypothyroidism, which requires lifelong medication. Radioiodotherapy can also lead to the development of hypothyroidism, and there is also a risk of recurrence of thyrotoxicosis. Drug treatment can lead to persistent remission in 35-50% of cases.
4. How does hyperthyroidism affect weight?
A typical symptom is weight loss despite a good or even increased appetite, due to an accelerated metabolism.
5. What are the dangers of hyperthyroidism if left untreated?
Without treatment, it is dangerous with serious heart problems, bone destruction (osteoporosis), and the risk of developing a deadly condition called thyrotoxic crisis.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Can AS, Rehman A. Goiter. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK562161/
3.
Pokhrel B, Bhusal K. Graves Disease [Internet]. StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK448195/
4.
Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, Rivkees SA, Samuels MH, Sosa JA, Stan MN, Walter MA. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016 Oct;26(10):1343-1421.
5.
Vanushko VE, Fadeev BB. Graves’ disease (clinical lecture). Problems of Endocrinology. 2013;59(2):59-68.
6.
Petunina NA, Trukhina LV, Martirosyan NS. Graves’ disease: a modern view on treatment issues. Effective pharmacotherapy. Endocrinology. 2010;(3):16-22.