Congenital Anomalies of Thyroid Gland: Classification, Clinical Manifestations, Diagnosis, and Treatment
Svetlana D.Surgical oncologist, MD
18 min read·September 01, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Congenital anomalies of the thyroid gland represent a heterogeneous group of congenital thyroid pathologies caused by disturbances during embryogenesis.
3D Models of Congenital Anomalies of Thyroid Gland:
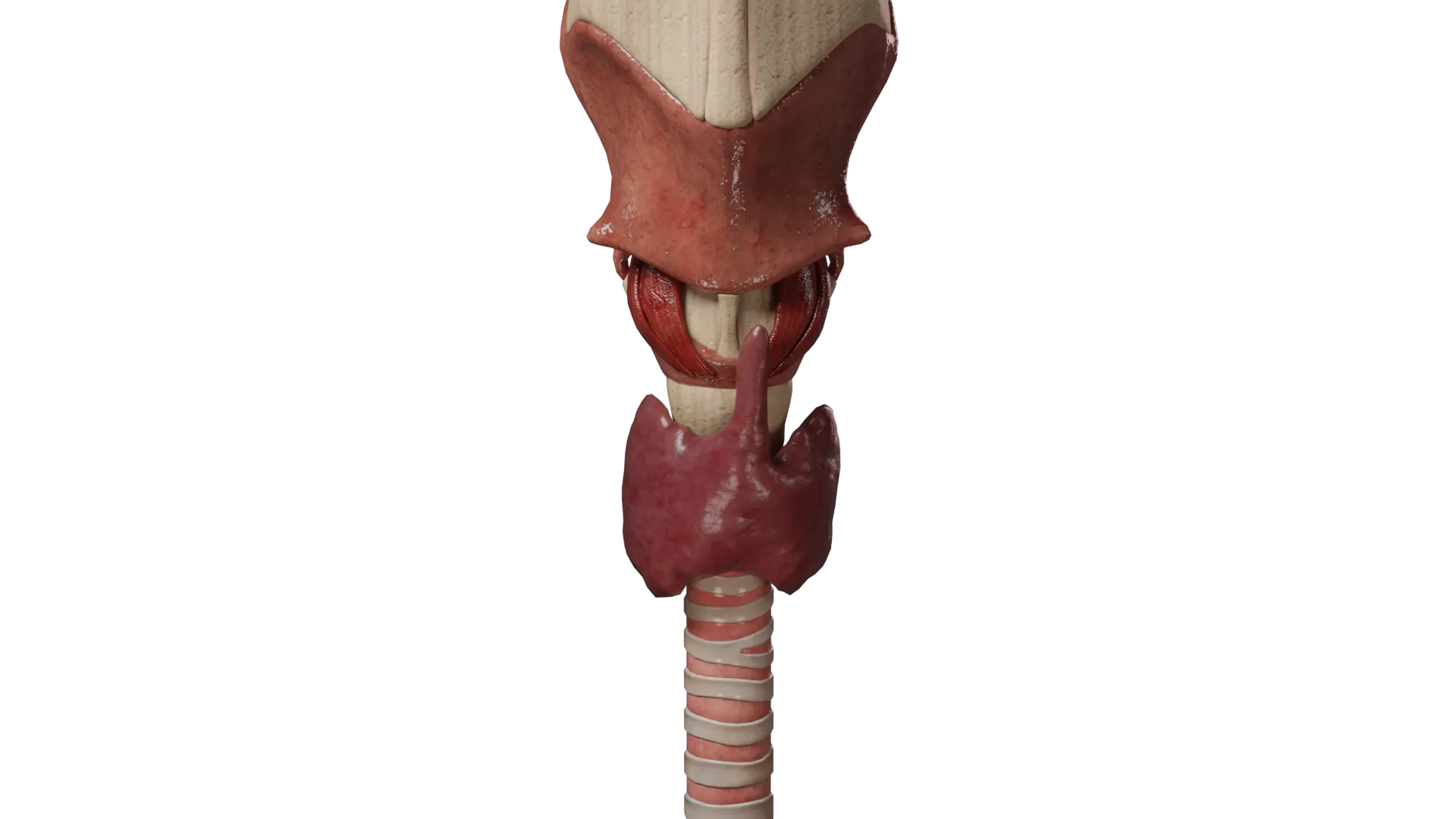
Aplasia of Left Lobe of Thyroid Gland
Lingual Ectopic Thyroid Gland
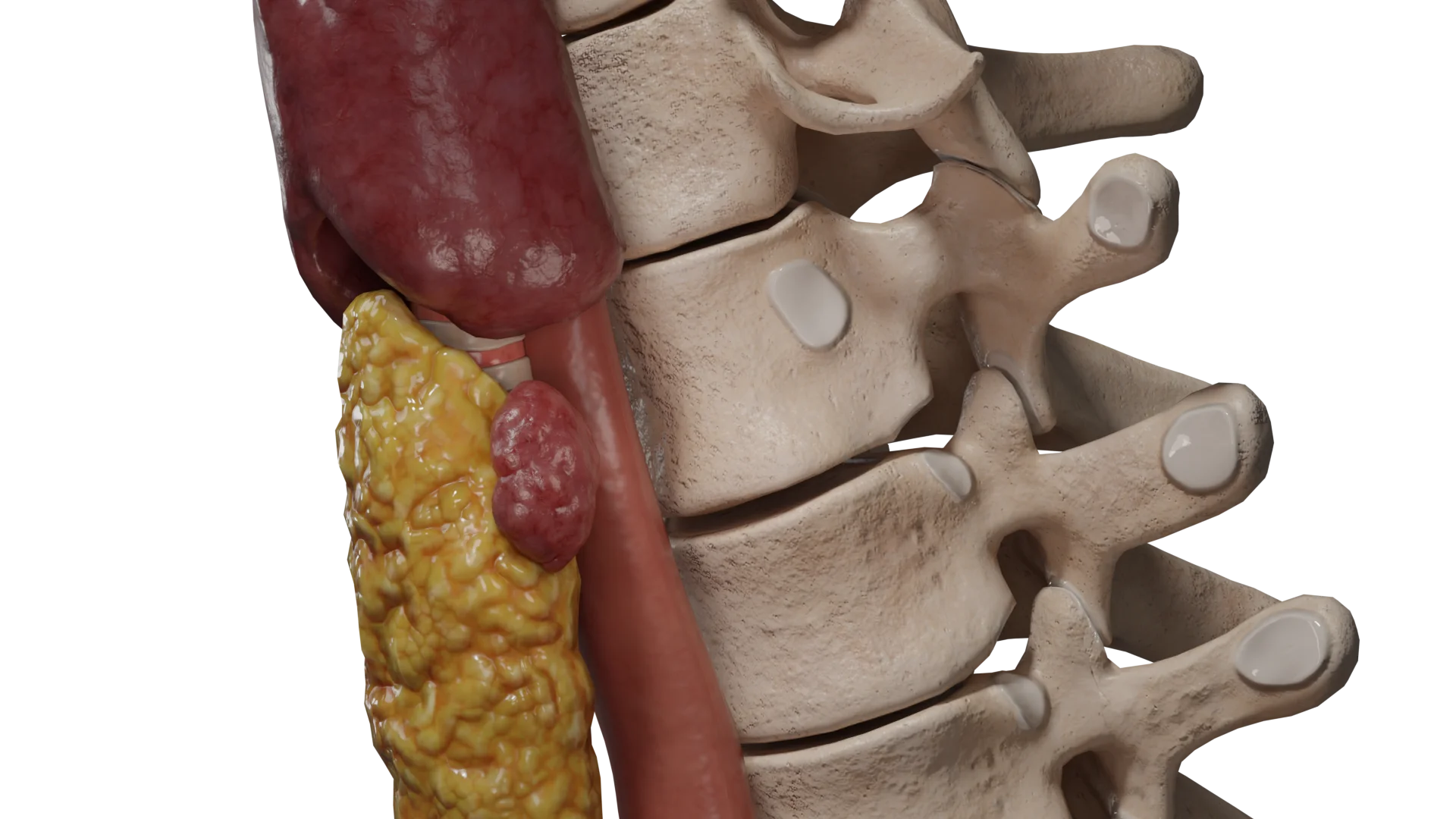
Accessory Lobe of Thyroid Gland
Embryology
The thyroid primordium appears during Weeks 3–4 of gestation from the endoderm between the first and second branchial arches at the base of the tongue and is connected to the pharynx via the thyroglossal duct.
Beginning in Week 5, the thyroid primordium migrates along the thyroglossal duct — from the root of the tongue caudally along the midline to its final position. During migration, the thyroid gland remains connected to the tongue by the thyroglossal duct, which normally obliterates completely by Week 8 of gestation.
Week 5 of gestation is also marked by the division of the thyroid gland into right and left lobes. At the same time, the ultimobranchial bodies form from the fourth and fifth branchial arches. These structures ultimately differentiate into parafollicular C-cells.
The ultimobranchial bodies fuse with the superior dorsolateral aspect of the developing thyroid gland, forming the Zuckerkandl’s tubercle. Parafollicular C-cells then disseminate into the thyroid gland but are typically concentrated in its superolateral aspects.
Mature C-cells secrete calcitonin, which lowers serum calcium levels by inhibiting osteoclast activity.
Cells continue to differentiate and mature from Week 7 to Week 12 of gestation; during this period, the thyroid gland becomes fully functional and begins synthesizing thyroid hormones.
Disruption of embryogenesis at any of the stages described above can lead to thyroid gland anomalies.
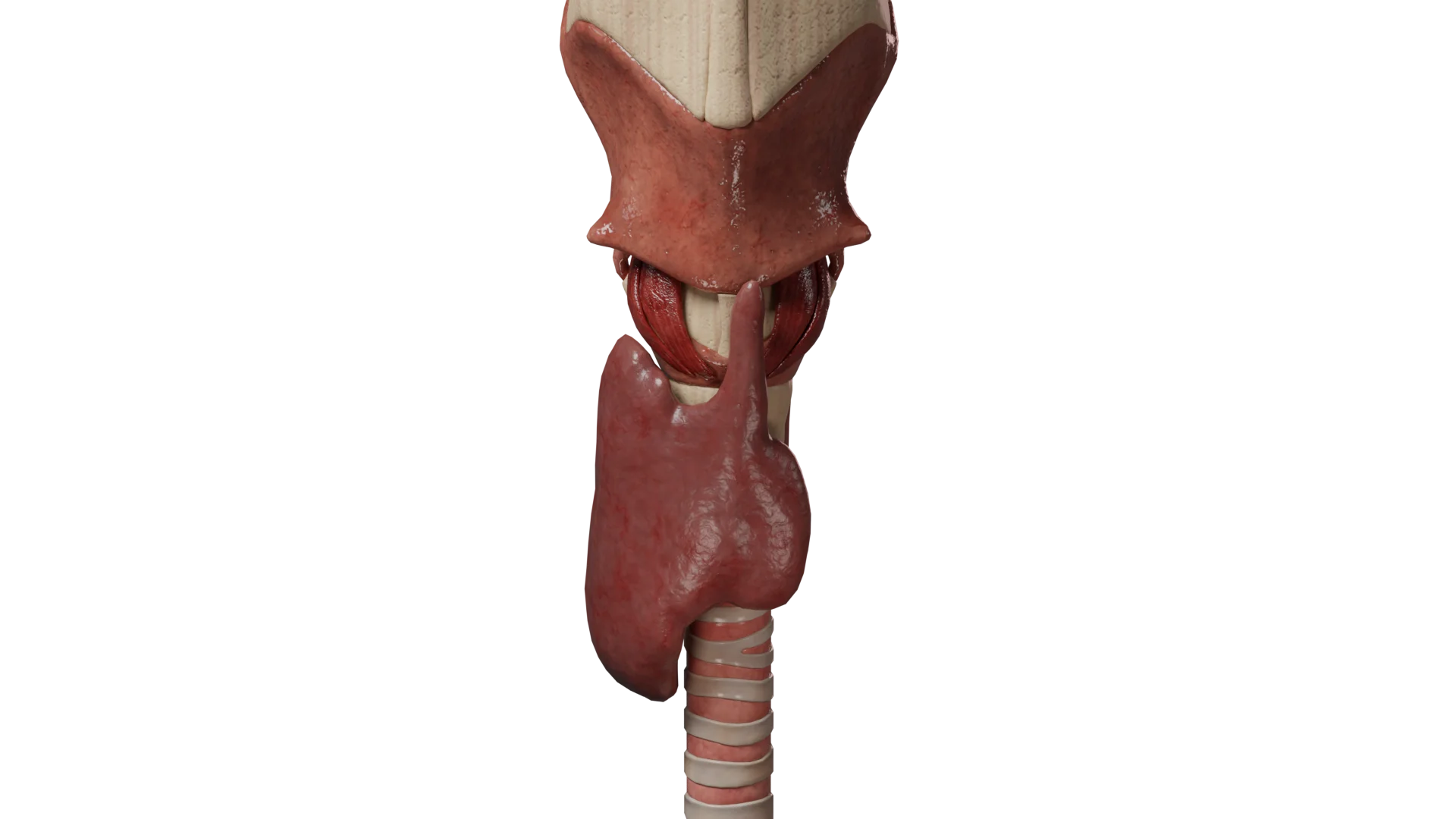
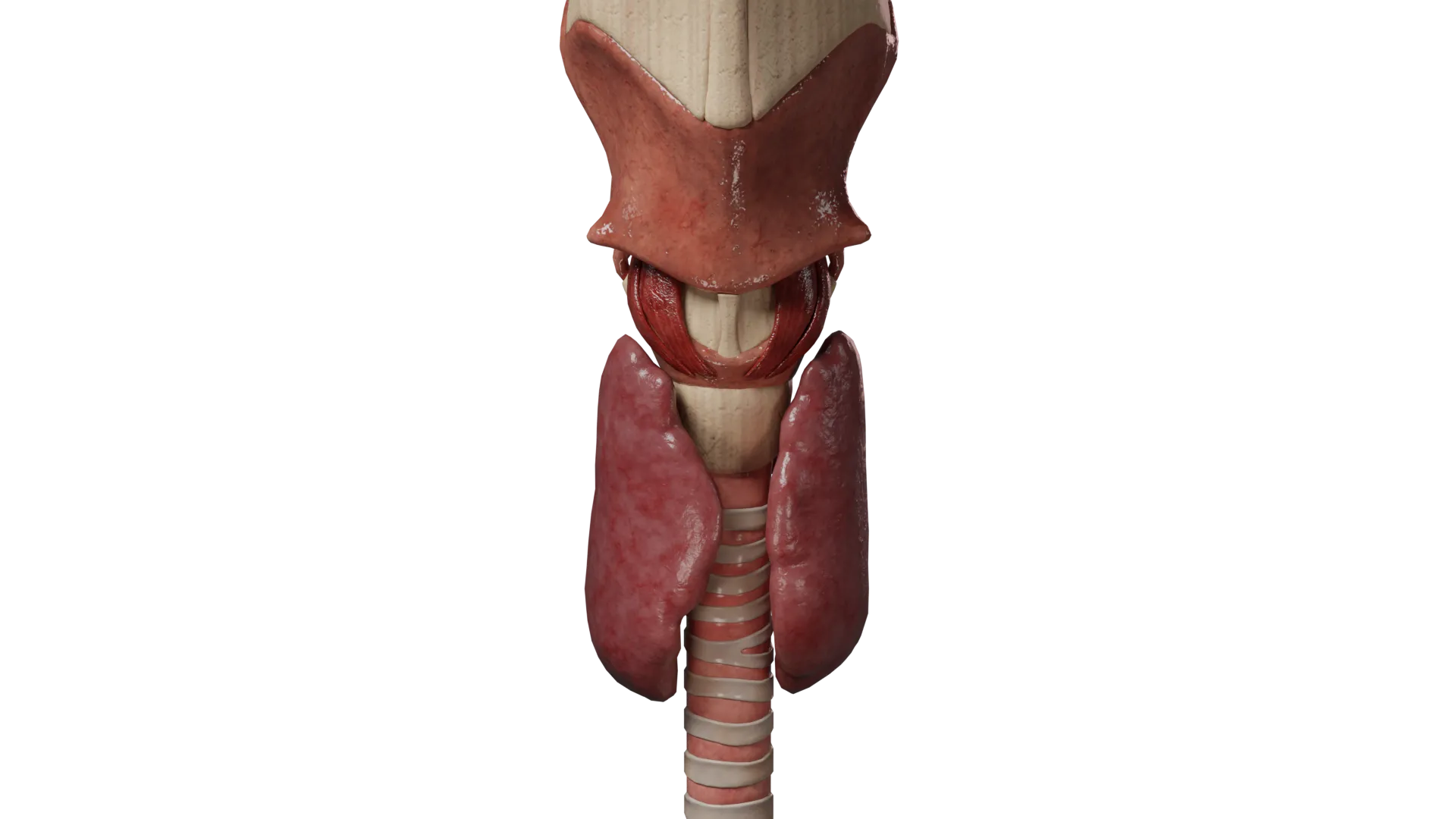
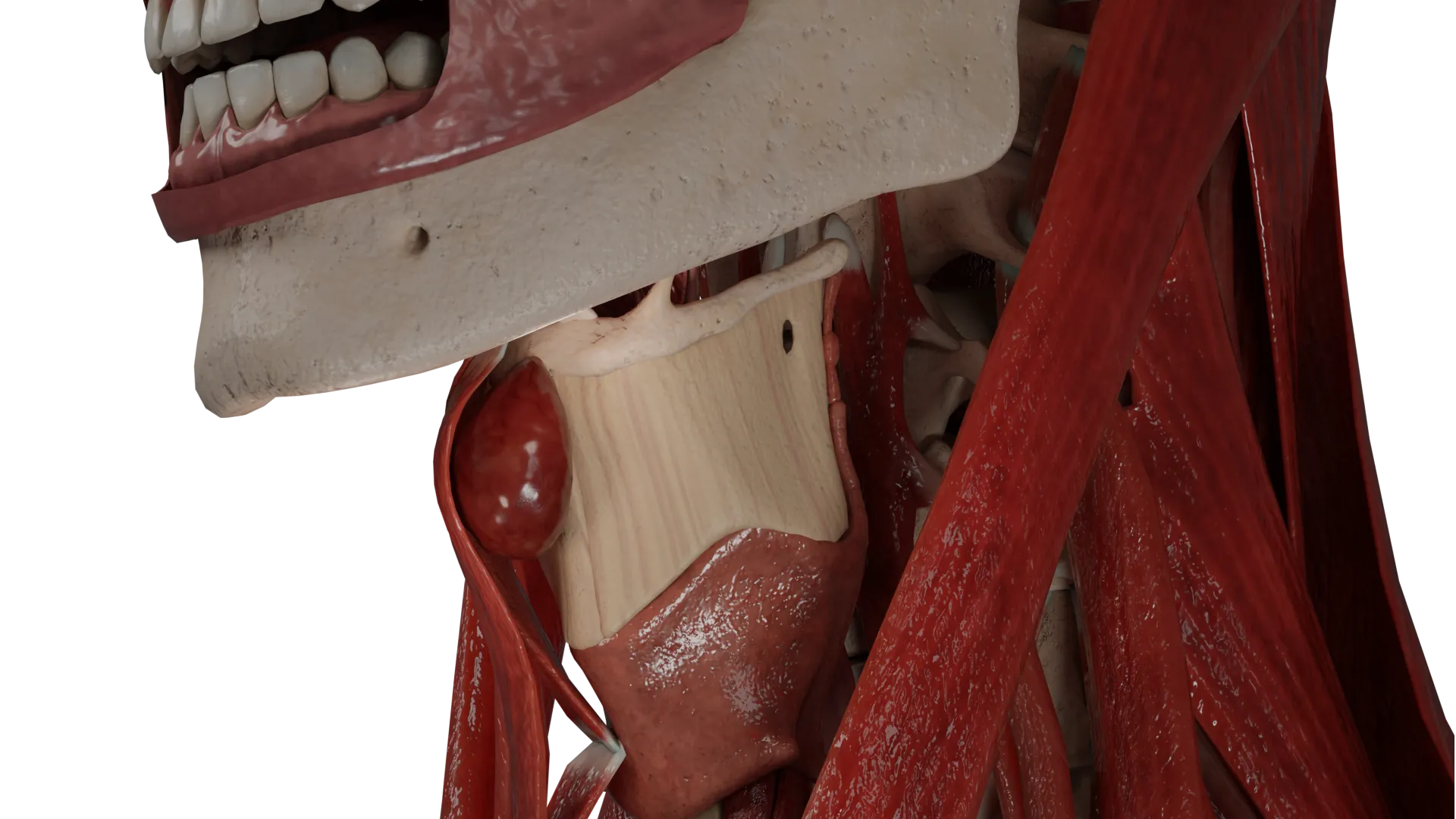
Anatomy
The thyroid gland is an endocrine organ located on the anterior surface of the neck, in front of the trachea, at the level of C5–T1. It comprises right and left lobes connected by an isthmus. A thin projection known as the pyramidal lobe may extend upward from the isthmus toward the hyoid bone.
The thyroid gland is attached to the trachea by the suspensory ligament (Berry’s ligament). The posterior surface of each lobe contains pyramidal enlargements called the Zuckerkandl’s tubercles, which mark the site of fusion of the ultimobranchial bodies with thyroid tissue.
Along with the pharynx, esophagus, and trachea, the thyroid gland is enclosed by the pretracheal fascia.
The thyroid gland receives arterial blood supply from the right and left superior thyroid arteries (branches of the external carotid arteries) and the right and left inferior thyroid arteries (branches of the thyrocervical trunk). In approximately 5 % of individuals, an additional unpaired artery, a. thyroidea ima, may be present. It may originate from the brachiocephalic trunk, subclavian artery, or aortic arch.
Venous drainage occurs through venous plexuses into the right and left superior and middle thyroid veins, which drain into the internal jugular veins, and the right and left inferior thyroid veins, which drain into the brachiocephalic veins.
Lymphatic drainage occurs via the pretracheal and paratracheal lymph nodes, then the jugular lymph nodes, and subsequently the right lymphatic duct and thoracic duct.
Innervation:
Sympathetic nerve fibers originate from the superior cervical ganglion and form the superior and inferior thyroid nerves;
Parasympathetic innervation is provided by branches of the right and left vagus nerves, specifically the superior laryngeal and recurrent laryngeal nerves.
Classification of Congenital Anomalies of Thyroid Gland
Thyroid dysgenesis:
Aplasia;
Hypoplasia;
Agenesis;
Ectopia.
Thyroglossal Duct Anomalies:
Thyroglossal duct cyst;
Accessory lobe of thyroid gland.
Thyroid dysgenesis
Clinical Manifestations of Thyroid Dysgenesis
Thyroid dysgenesis is the most common congenital pathology of the endocrine system, with an incidence ranging from 1 : 4,000 to 1 : 7,000 live births. According to statistics, up to 85 % of cases of congenital hypothyroidism can be attributed to thyroid dysgenesis.
Risk factors for thyroid dysgenesis are as follows:
Genetic predisposition: so far, mutations in the TSHR, PAX8, FOXE1, and NKX2-1 genes have been shown to be associated with dysgenesis;
Intrauterine infections;
Ionizing radiation during pregnancy;
Exposure to chemical toxins and pharmacological agents during pregnancy;
Iodine deficiency in the maternal diet during pregnancy;
Maternal autoimmune diseases during pregnancy, accompanied by hypothyroidism.
Thyroid dysgenesis may present in various forms, including:
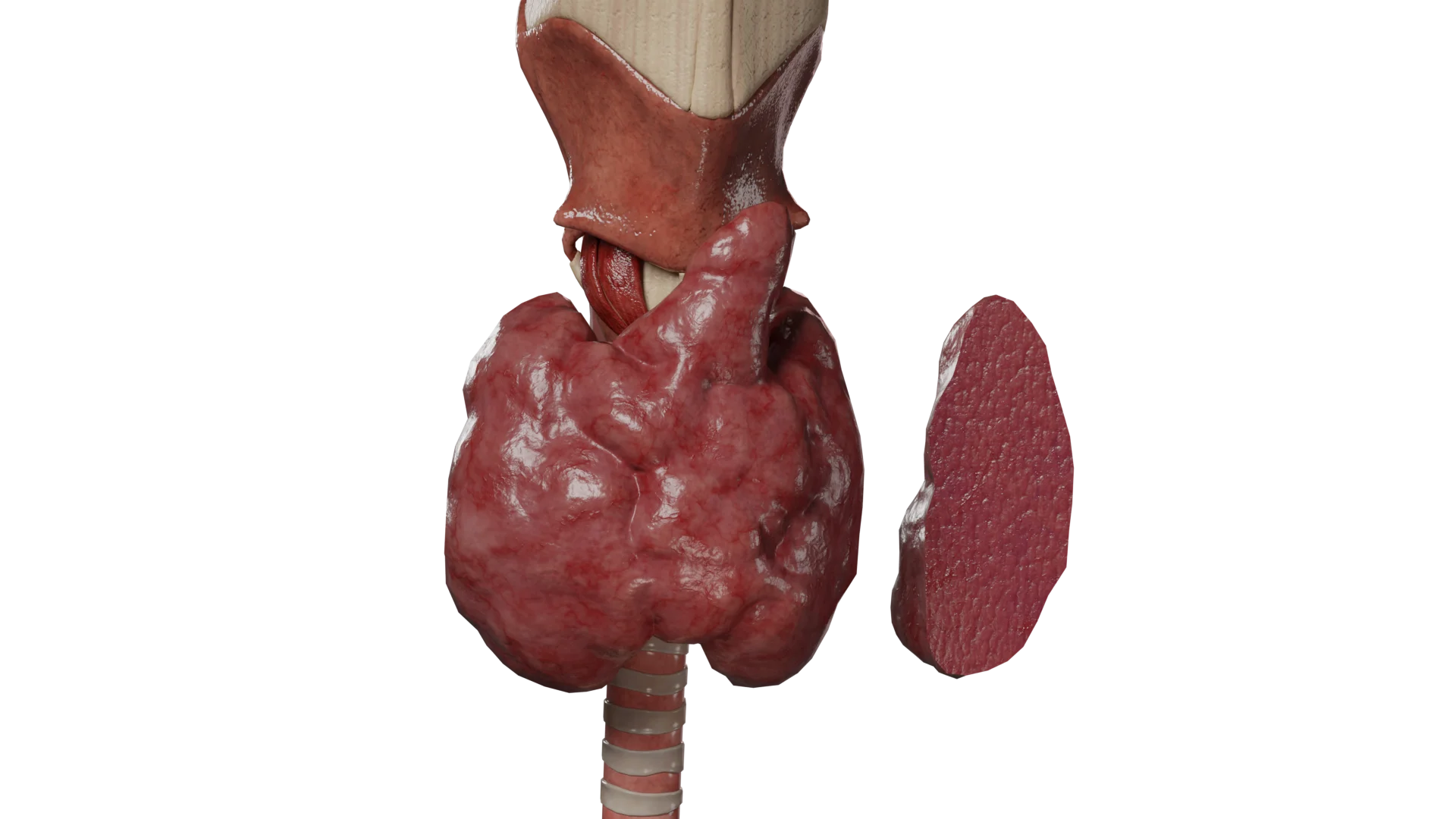
Aplasia means that the thyroid gland or one of its lobes (either right or left) is completely absent. This pathology is also referred to as thyroid hemiagenesis.
3D Animation — Aplasia of Left Lobe of Thyroid Gland
Thyroid aplasia is responsible for congenital hypothyroidism.
Typical hypothyroidism features are observed in only 10–15 % of newborns due to the transfer of maternal thyroxine through the bloodstream. Clinical manifestations tend to develop gradually over the course of six weeks of life, although severe cases may present earlier.
Muscle hypotonia: a protuberant abdomen with a umbilical hernia; diastasis of rectus abdominis muscles;
Hyporeflexia;
Frequent constipation;
Cold, dry, mottled skin;
Dry, brittle hair; seborrhea of the scalp, forehead, and eyelids;
Respiratory disturbances due to mucosal edema of the airways: stridor, nasal obstruction, cyanosis of the nasolabial triangle.
In children older than 5–6 months, symptoms of psychomotor and intellectual developmental delay become predominant. Growth arrest is also observed, leading to pronounced short stature.
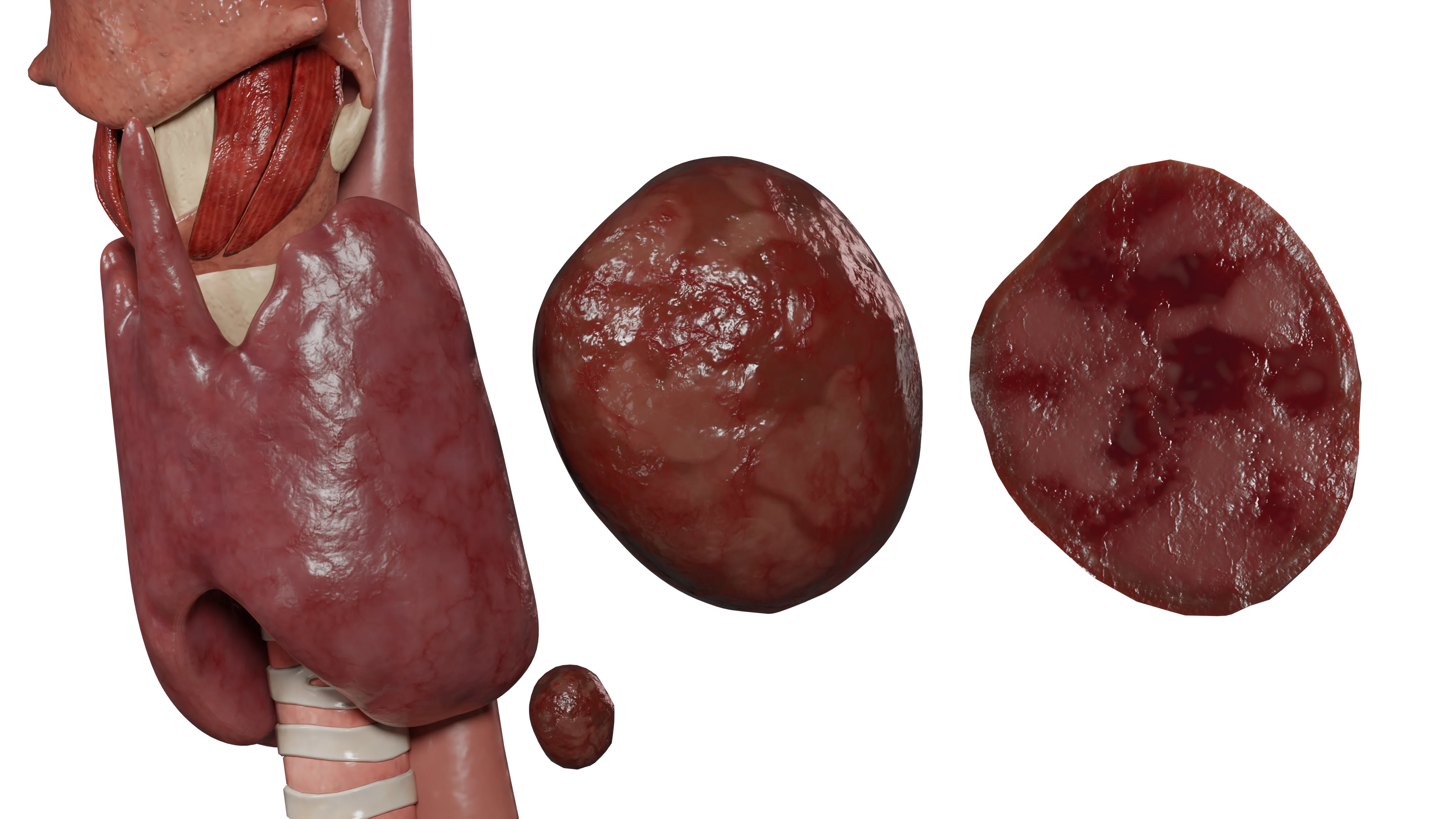
Hypoplasia is a reduction in the volume and size of the thyroid gland caused by underdeveloped thyroid tissue.
Thyroid Hypoplasia — 3D Animation
Thyroid hypoplasia, similar to aplasia, leads to congenital hypothyroidism. The severity of thyroid insufficiency correlates with the degree of underdevelopment of thyroid tissue.
Ectopic thyroid gland refers to thyroid tissue located in an atypical position. The most common form is lingual ectopia; however, in rare cases, thyroid tissue may be found within nearby structures (trachea, larynx, mediastinum) or in distant anatomical sites (intestine, ovaries).
3D Animation — Lingual Ectopic Thyroid Gland
In 7–10 % of cases, ectopia may be asymptomatic and detected only by ultrasound, CT, or MRI.
Most cases of thyroid ectopia (up to 70 %) lead to hypothyroidism; in such cases, thyroid tissue maturity determines the severity of clinical manifestations.
Hyperthyroidism accounts for approximately 20 % of cases. Typical symptoms of thyrotoxicosis include:
Weight gain despite reduced appetite;
Bradycardia;
Marked weakness and fatigue;
Somnolence;
Facial and limb edema;
Constipation;
Dry skin.
In addition to symptoms related to altered thyroid hormone production, patients with thyroid ectopia often present with complaints associated with the abnormal location of thyroid tissue.
In lingual ectopia, commonsymptoms may include:
Sore throat;
Globus sensation;
Cough;
Dysphagia;
Dysphonia;
Possible sleep apnea.
Frequent trauma may lead to complications such as recurrent bleeding, abscess, and, in rare cases (up to 1 %), malignant transformation of ectopic thyroid tissue.
In patients with ectopic thyroid tissue in the trachea, larynx, or mediastinum, complaints may include dyspnea, tachypnea, and cyanosis of the nasolabial triangle. In rare cases, airway obstruction may occur, leading to asphyxia and death.
Diagnosis of Thyroid Dysgenesis
Medical history and physical examination. An initial evaluation may reveal characteristic symptoms of hypothyroidism or thyrotoxicosis. In lingual ectopia, laryngoscopy allows visualization of thyroid tissue without the need for instrumental diagnostic methods.
Laboratory tests. Thyroid hormone blood levels — thyroid-stimulating hormone (TSH) and thyroxine (free T4 and total T4) — enable assessment of thyroid function and the severity of hypothyroidism or thyrotoxicosis. Additional tests specify levels of thyroglobulin (Tg), triiodothyronine (T3 and free T3), anti-thyroid peroxidase antibodies (anti-TPO), anti-TSH receptor antibodies (TRAb), and anti-thyroglobulin antibodies (anti-Tg).
Imaging methods:
Ultrasound (US) helps visualize thyroid tissue.
This method is simple, safe, suitable for patients of any age, and has high sensitivity and specificity. However, it is less effective in diagnosing thyroid ectopia.
Scintigraphy (using I-123 and Tc-99m radionuclides) is a highly sensitive and informative method for assessing the localization and functional activity of thyroid tissue. Contraindications include pregnancy, breastfeeding, individual intolerance to radiopharmaceuticals, severe renal or hepatic insufficiency, and fever.
Computed tomography (CT) or magnetic resonance imaging (MRI) may also be used.
Treatment of Thyroid Dysgenesis
Therapy for thyroid dysgenesis includes both medical and surgical approaches.
Asymptomatic cases (typically in patients with agenesis of the thyroid isthmus) do not require treatment, since there are no hormonal disturbances.
Medical therapy
Hormone Replacement Therapy (HRT)
In cases of aplasia, hypoplasia, or ectopia of the thyroid gland, the cornerstone of treatment is correction of congenital hypothyroidism through hormone replacement therapy (HRT) with levothyroxine sodium. Early diagnosis and therapy are critically important, as thyroid insufficiency in infants and young children leads to irreversible intellectual and psychomotor developmental disorders.
The starting levothyroxine sodium dose is determined according to age-related requirements for thyroxine:
Newborns — 10–15 µg/kg body weight;
Children — 2–2.5 µg/kg body weight;
Adults — 1.5–1.6 µg/kg body weight.
The dose of thyroxine is adjusted based on serum thyroid hormone levels until a euthyroid state is achieved.
Therapy for Hyperthyroidism
In thyroid ectopia with hyperthyroidism, antithyroid (thyrostatic) therapy is indicated. Thionamides (methimazole, propylthiouracil) and glucocorticoid hormones are employed. Doses are determined individually, depending on the severity of thyrotoxicosis. In patients with tachycardia, beta-blockers are prescribed to reduce heart rate and decrease the risk of arrhythmias.
Thyrotoxicosis may be treated with radioiodine therapy (RIT). RIT feasibility and the radiopharmaceutical dose are determined individually.
Surgical therapy
Surgical intervention is indicated in the following cases:
Ineffective conservative therapy for thyrotoxicosis;
Symptoms such as dysphagia, dysphonia, dyspnea, or compression of adjacent organs by ectopic thyroid tissue;
Frequent trauma to the tissue with recurrent bleeding or abscess formation;
A benign tumor in ectopic tissue and/or suspected malignancy.
Gross total resection of ectopic thyroid tissue within healthy margins is performed, followed by HRT with levothyroxine sodium. This is necessary when the ectopic gland is the only thyroid tissue present or when the normally located thyroid gland is functionally impaired.
Thyroglossal Duct Anomalies
Clinical Manifestations of Thyroglossal Duct Anomalies
This group of congenital anomalies of the thyroid gland is caused by incomplete obliteration of the thyroglossal duct during the embryonic period.
A thyroglossal duct cyst is a nonneoplastic, fluid-filled lesion located on the anterior surface of the neck, closely associated with the body of the hyoid bone.
Small cysts are typically asymptomatic. Patients with cysts larger than 5 mm present with an elastic, rounded midline neck mass that is mobile during swallowing and generally painless.
Infection of the cyst occurs in 20–60 % of cases and is accompanied by:
Increase in cyst size;
Pain in the affected area;
Local erythema of the skin;
Possible fever;
A possible fistulous tract opening onto the anterior surface of the neck.
In rare cases (1–2 %), malignant transformation may occur.
An accessory lobe of the thyroid gland is an additional area of thyroid tissue separate from the normally located thyroid gland.
In most cases, an accessory lobe is asymptomatic and detected incidentally during routine ultrasound examination.
When the accessory lobe is large, symptoms of compression of adjacent organs may develop:
Globus sensation;
Dysphagia;
Hoarseness;
Dyspnea.
Hyperthyroidism may occur due to functional autonomy of the aberrant lobe, accompanied by typical clinical manifestations.
Diagnosis of Thyroglossal Duct Anomalies
The diagnostic approach to thyroglossal duct anomalies employs the same laboratory and imaging modalities used for thyroid dysgenesis.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of Thyroglossal Duct Anomalies
Thyroglossal duct cysts require surgical treatment. Isolated excision of such cysts is currently considered inappropriate due to a high recurrence risk, reported to be up to 50 % in some sources.
The gold standard for surgical treatment of thyroglossal duct cysts is the Sistrunk procedure. The cystic cavity is removed along with the body of the hyoid bone (to which the cyst is closely attached). If the thyroglossal duct persists along its entire course, excision of tissue at the tongue root is also performed. The recurrence risk after the Sistrunk procedure is less than 10 %.
An asymptomatic accessory lobe does not require treatment. Surgical removal of the accessory lobe is indicated in cases of compression of surrounding organs or hyperthyroidism due to functional autonomy of the accessory lobe. This may be demonstrated by hyperfixation of radiopharmaceuticals on scintigraphy, with normal or reduced uptake by normally located thyroid tissue.
FAQ
1. What is thyroid hypoplasia?
Thyroid hypoplasia is a congenital condition in which the gland fails to reach normal size during embryonic development and remains smaller than expected. This may impair its function and lead to hypothyroidism. In cases of hypoplasia affecting only one lobe (either right or left), the other lobe may develop to normal size or become slightly enlarged to maintain hormonal function. The phenomenon is known as compensatory hyperplasia. Thyroid endocrine function in such cases may remain unaffected or may be impaired, resulting in hypothyroidism.
2. What causes congenital anomalies of the thyroid gland?
Congenital anomalies of the thyroid gland may be caused by genetic factors, including mutations in specific genes. In addition, environmental influences — such as intrauterine infections, ionizing radiation, iodine deficiency, toxic substances, or medications during pregnancy — may provoke the condition. Maternal autoimmune diseases can additionally affect thyroid development in the fetus.
3. How are thyroid gland anomalies diagnosed?
Diagnosis includes ultrasound, scintigraphy, and CT/MRI for visualization of thyroid tissue, as well as laboratory tests for thyroid hormone levels to evaluate thyroid function and determine the severity of hypothyroidism or thyrotoxicosis.
4. How are they treated?
Treatment may include medical and surgical therapy. The former involves HRT for hypothyroidism correction or antithyroid for hyperthyroidism. The latter implies removal of an accessory thyroid lobe or a thyroglossal duct cyst.
References
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Mutation of the gene encoding human TTF-2 associated with thyroid agenesis, cleft palate and choanal atresia (R.J. Clifton-Bligh, J.M. Wentworth, P. Heinz, M.S. Crisp, R. John, J.H. Lazarus, M. Ludgate, V.K. Chatterjee).
https://www.ncbi.nlm.nih.gov/books/
3.
Anatomy, Head and Neck, Thyroid (Evan Allen; Abbey Fingeret).
https://www.ncbi.nlm.nih.gov/books/
4.
Клинические рекомендации «Врожденный гипотиреоз» (Петеркова В А, Безлепкина О Б, Ширяева Т Ю, Вадина Т А, Нагаева Е В, Чикулаева О А, Шредер Е В, Конюхова М Б, Макрецкая Н А, Шестопалова Е А, Митькина В Б). [Klinicheskie rekomendatsii «Vrojdennyiy gipotireoz» (Guidelines for Congenital Hyperthyroidism) (Peterkova V A, Bezlepkina O B, SHiryaeva T YU, Vadina T A, Nagaeva E V, CHikulaeva O A, SHreder E V, Konyuhova M B, Makretskaya N A, SHestopalova E A, Mitkina V B)]
https://www.ncbi.nlm.nih.gov/
5.
Congenital Hypothyroidism (Sasigarn A. Bowden; Marina Goldis).
https://www.ncbi.nlm.nih.gov/books/
6.
Thyroglossal Duct Cyst (Janine Amos; Carl Shermetaro).
https://www.ncbi.nlm.nih.gov/books/
7.
2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis.
8.
Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement (2014).