The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
A craniocerebral injury (CCI) is damage to the bones of the cranial vault or skull base, as well as to the brain itself, resulting from the impact of external mechanical factors on the head region.
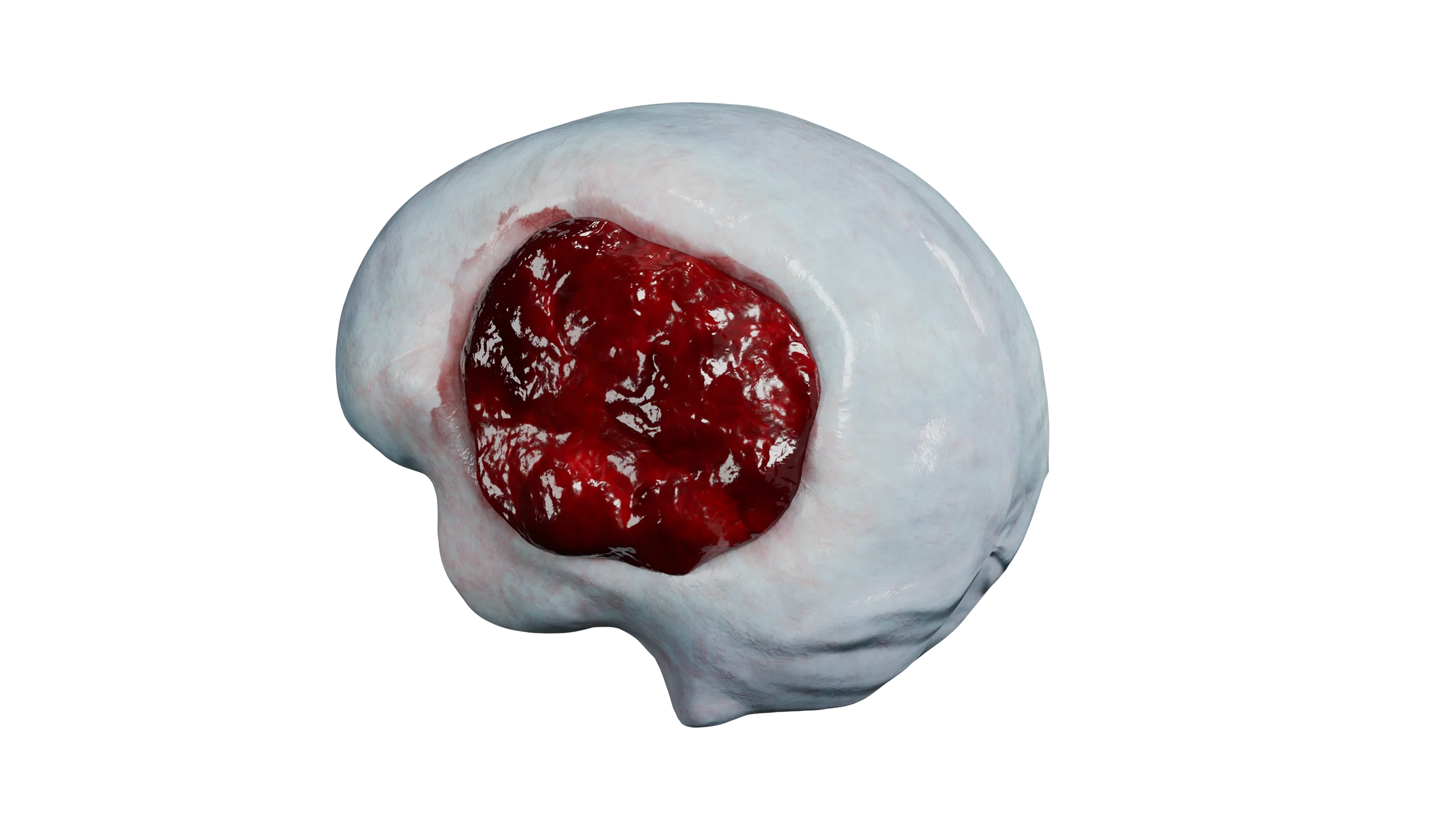
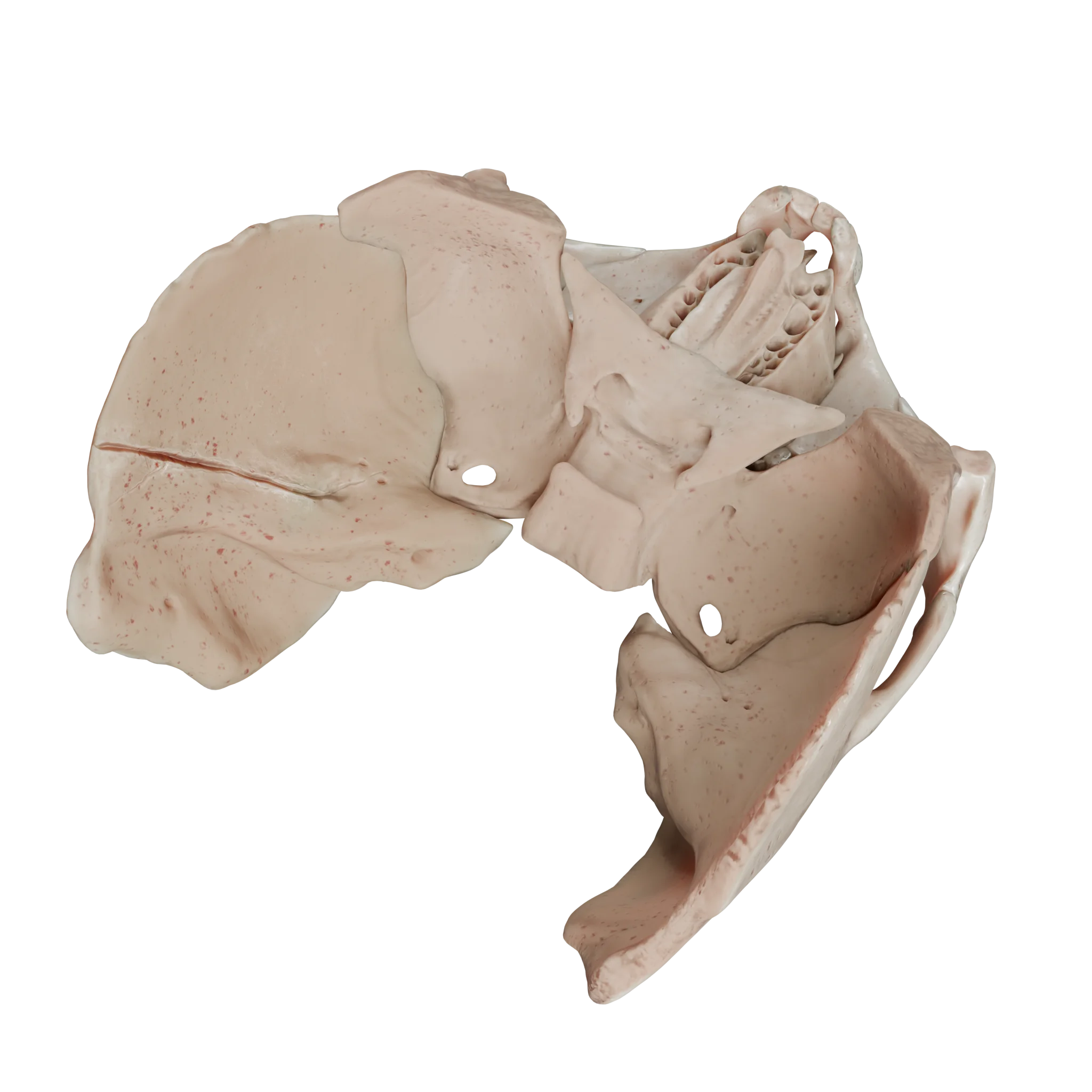
Impression fracture of the cranial vault bones – 3D Model
Epidemiology of traumatic brain injury
Current trends in traumatic brain injury include affecting the young able-bodied population, high rates of disability and mortality, and significant costs of treatment of patients with this pathology. Every year, 27 million new cases of traumatic brain injury are recorded worldwide, which is about 400 cases per 100,000 population.
According to age categories, PMT can be categorized into:
Infant traumatic brain injury, often associated with a baby falling;
Adolescent and adult traumatic brain injury, where the primary cause of injury is motor vehicle accidents;
PMT in old age, where falls are the most common cause of injury.
In addition, there are gender differences in the structure of traumatic brain injury: men are injured twice as often as women (on average).
The severity of traumatic brain injury is evidenced by the high mortality rate: about 10 people per 100,000 population die from traumatic brain injury each year, with about 70% of patients dying before receiving qualified medical care.
Etiology of traumatic brain injury
The most common etiologic factors of traumatic brain injury:
Falls (40-50% of all head injuries);
Road traffic accidents (20-30% of all head injuries);
Intentional infliction of bodily harm;
Occupational Injuries.
The contribution of various etiologic factors to the development of brain injury varies with the income of the country, geographic location, and political situation in a given region.
Pathogenesis of traumatic brain injury
The direct impact of various mechanical factors, which include shock-impact mechanism and acceleration-deceleration mechanism, can cause two types of primary brain damage, focal and diffuse.
Shock and impact mechanism
Shock-impact mechanism causes focal brain injury due to the impact of mechanical energy with a stiffened skull, which entails injury to the soft tissues of the head, skull bones and brain in the area of contact with the traumatic agent.
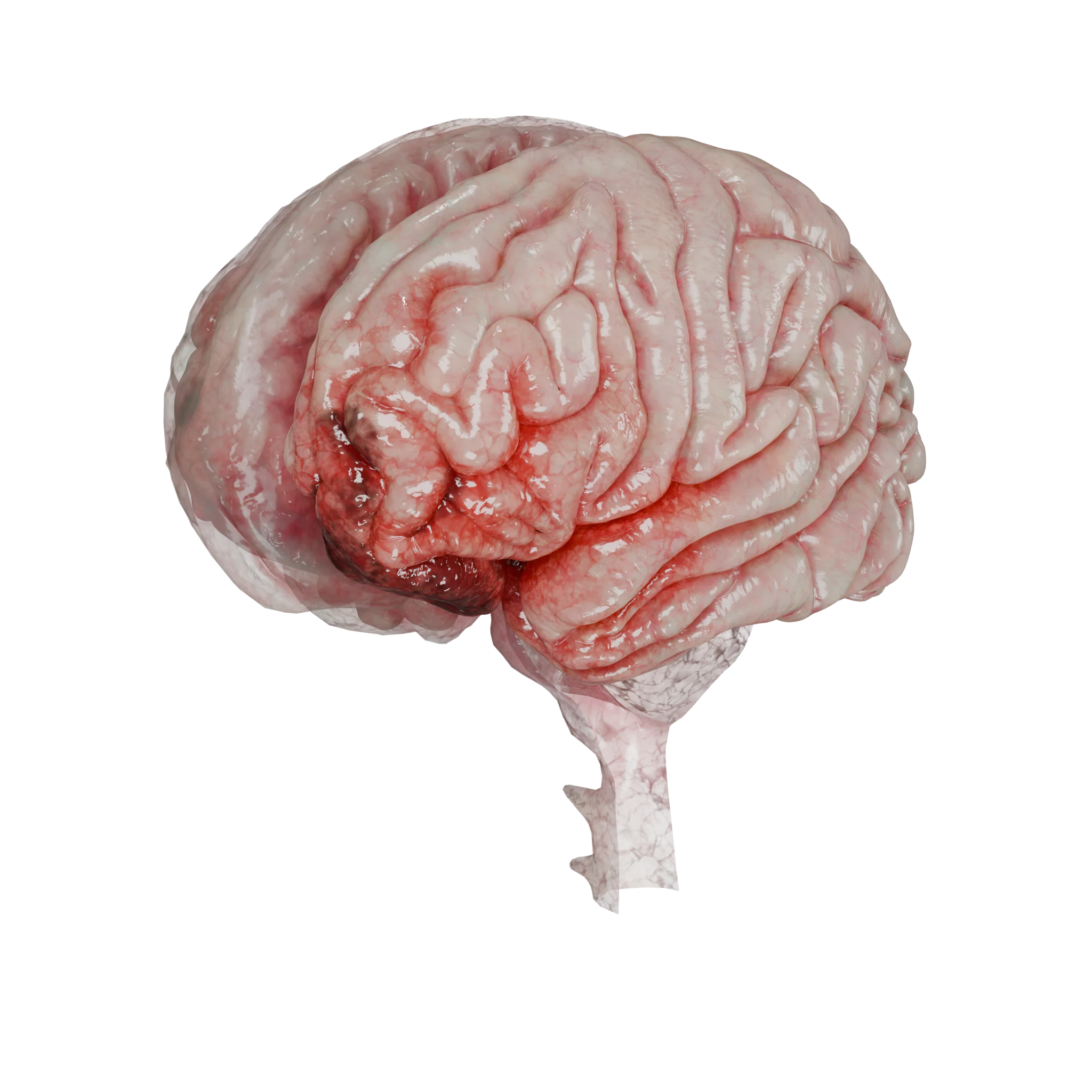
Due to biophysical features of the skull, there is a short-term decrease in pressure at the point of counter-impact, cavitation reactions are formed, which leads to traumatization of the brain at a point opposite to the point of trauma impact. This mechanism of traumatization underlies the pathogenesis of traumatic intracranial hematomas, brain contusions, skull bone fractures, traumatic subarachnoid hemorrhages, which are represented in our 3D Models:
Moderate cerebral contusion – 3D ModelAcute epidural hematoma of basal temporal localization – 3D Model
Acceleration-deceleration mechanism
The acceleration-deceleration mechanism is caused by the impact on the head of successive acceleration forces followed by a sharp deceleration. During this mechanical impact, microtrauma occurs in the area connecting the cerebral hemispheres and brainstem. This mechanism underlies the pathogenesis of concussion and diffuse axonal brain injury.
Classification of traumatic brain injury
By type of biomechanical effect
Shockproof;
Acceleration-deceleration.
By type of damage
Focal – based on an impact-impact mechanism of injury;
Diffuse – based on the acceleration-deceleration mechanism.
By the nature of the injury
Open – the presence of an aponeurosis injury;
Closed – the aponeurosis is intact;
Penetrating – damage to the dura mater;
Non-penetrating – the dura mater is intact.
By severity (Glasgow Coma Scale)
Light (13-15 points);
Medium (9-12 points);
Severe (3-8 points).
Clinical forms
Concussion;
Brain contusion:
Mild degree;
Medium Degree;
Severe degree.
Diffuse axonal damage;
Brain compression (acute, subacute, chronic).
By degree of recovery (Glasgow Outcome Scale)
Full recovery – complete restoration of the patient’s ability to work;
A good recovery is a small neurologic deficit that does not interfere with daily life;
Mild non-self – opportunity for change of occupation, special employment;
Moderate non-self-care – partial impairment of self-care;
Severe non-self – significant neurologic deficit requiring ongoing care;
Neuromuscular failure – need for continuous care in the NICU;
Vegetative state – maintaining wakefulness and sleep cycles with no signs of consciousness or contact;
Lethal is the death of the patient.
Clinical manifestations of traumatic brain injury
The symptomatology of craniocerebral injury (CCI) is very diverse and is determined by the severity of the injury and the localization of the focus in relation to important functional areas of the brain.
All types of traumatic brain injury are accompanied by a loss of consciousness, which can last from a few seconds to several days or even weeks, depending on the degree of brain damage.
Neurologic deficits of various types result from direct brain damage and are divided into general cerebral, focal, trunk, and meningeal symptoms.
The general cerebral symptoms include headache, impaired consciousness, dizziness, and vomiting, which are due to changes in intracranial pressure resulting in intracranial hypertension or hypotension.
Focal symptoms are associated with localized damage to areas of the brain responsible for specific functions. These include:
Mental disorders in damage to the basal portions of the frontal lobes.
Paresis or paralysis from damage to the motor cortex or cortico-spinal tracts.
Sensory disturbances with damage to the postcentral gyrus or conductive pathways.
Aphasic disturbances in Broca’s and Wernicke’s area damage.
Visual field loss with damage to the occipital lobes or optic radiating.
Stem symptoms in traumatic brain injury include damage to the midbrain, which is manifested by oculomotor disturbances and the development of bulbar syndrome (dysphonia, dysarthria, dysphagia) due to damage to the caudal nerve nuclei at the level of the brainstem.
Hypothalamic disorders occur when the hypothalamus is damaged due to basal brain contusions, massive intracranial hematomas, or skull base fractures. These symptoms are manifested by disturbances in blood osmolarity and autonomic disorders.
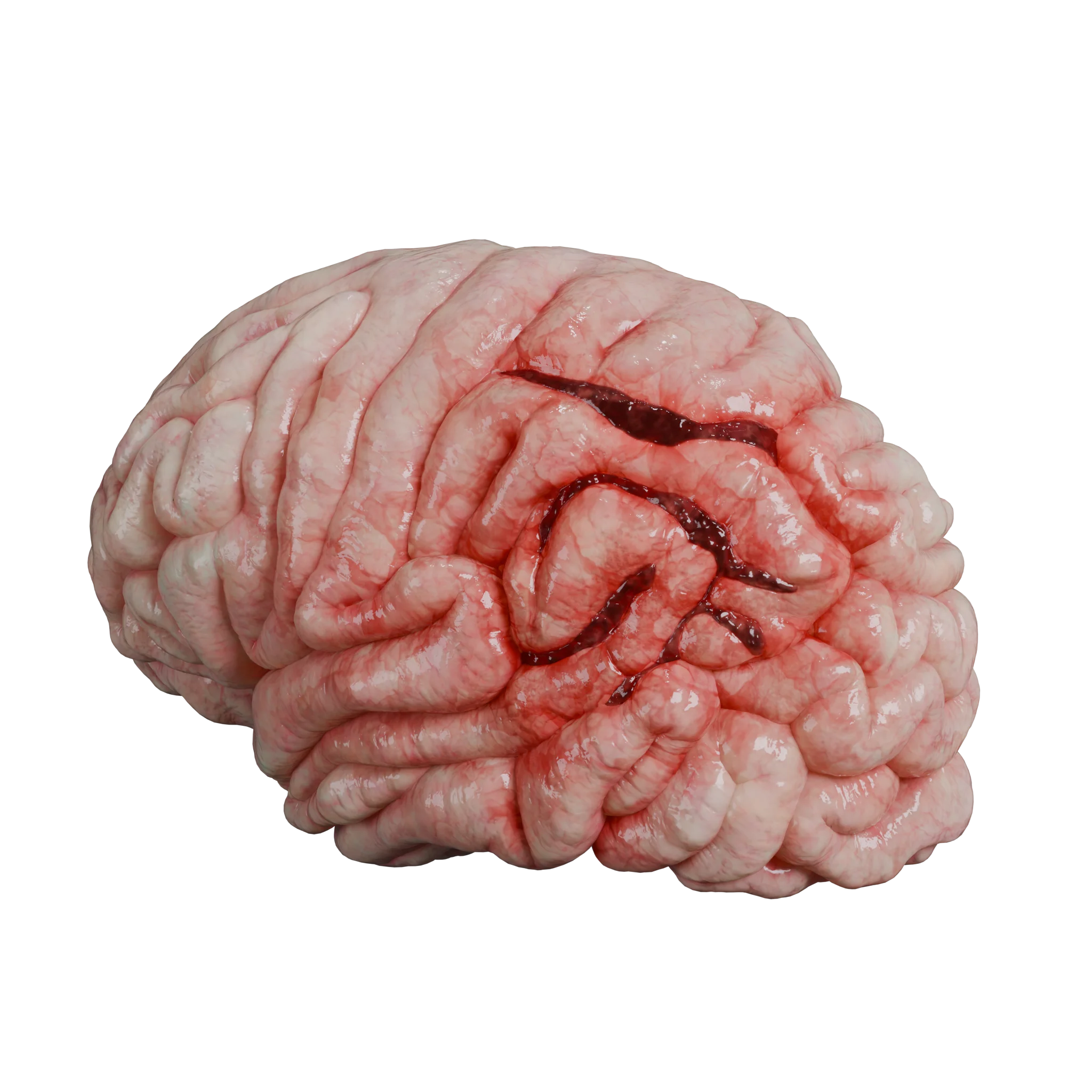
Meningeal symptoms are due to irritation of the cerebral membranes by intracranial hemorrhage and are manifested by stiffness of the occipital muscles, pathologic meningeal signs, pain on head percussion, and general hyperesthesia. These symptoms typically develop in traumatic subarachnoid hemorrhage, which is represented in the model below.
Traumatic subarachnoid hemorrhage in the left parietal lobe – 3D Model
Diagnosis of brain injuries
History taking
The first and most basic step in the diagnosis of traumatic brain injury is the collection of anamnesis. It is important to find out the mechanism of injury (fall from a height, impact, traffic accident) and the time elapsed since the accident. Determination of the mechanism of trauma suggests possible focal or diffuse brain damage (for example, a blow with a heavy object may lead to a fracture of the skull bones, and a road traffic accident with acceleration-deceleration – to diffuse axonal damage).
Physical Examination
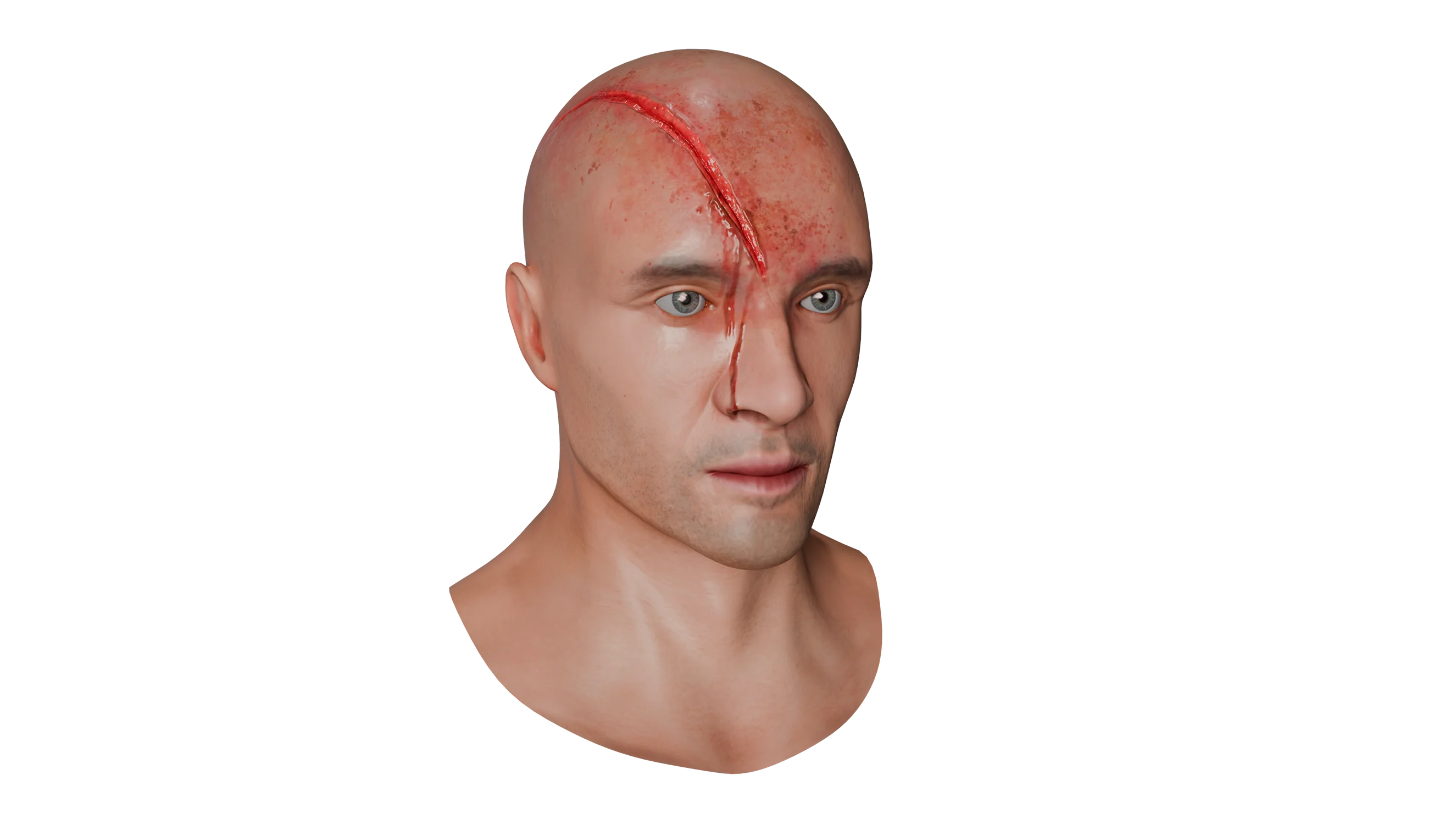
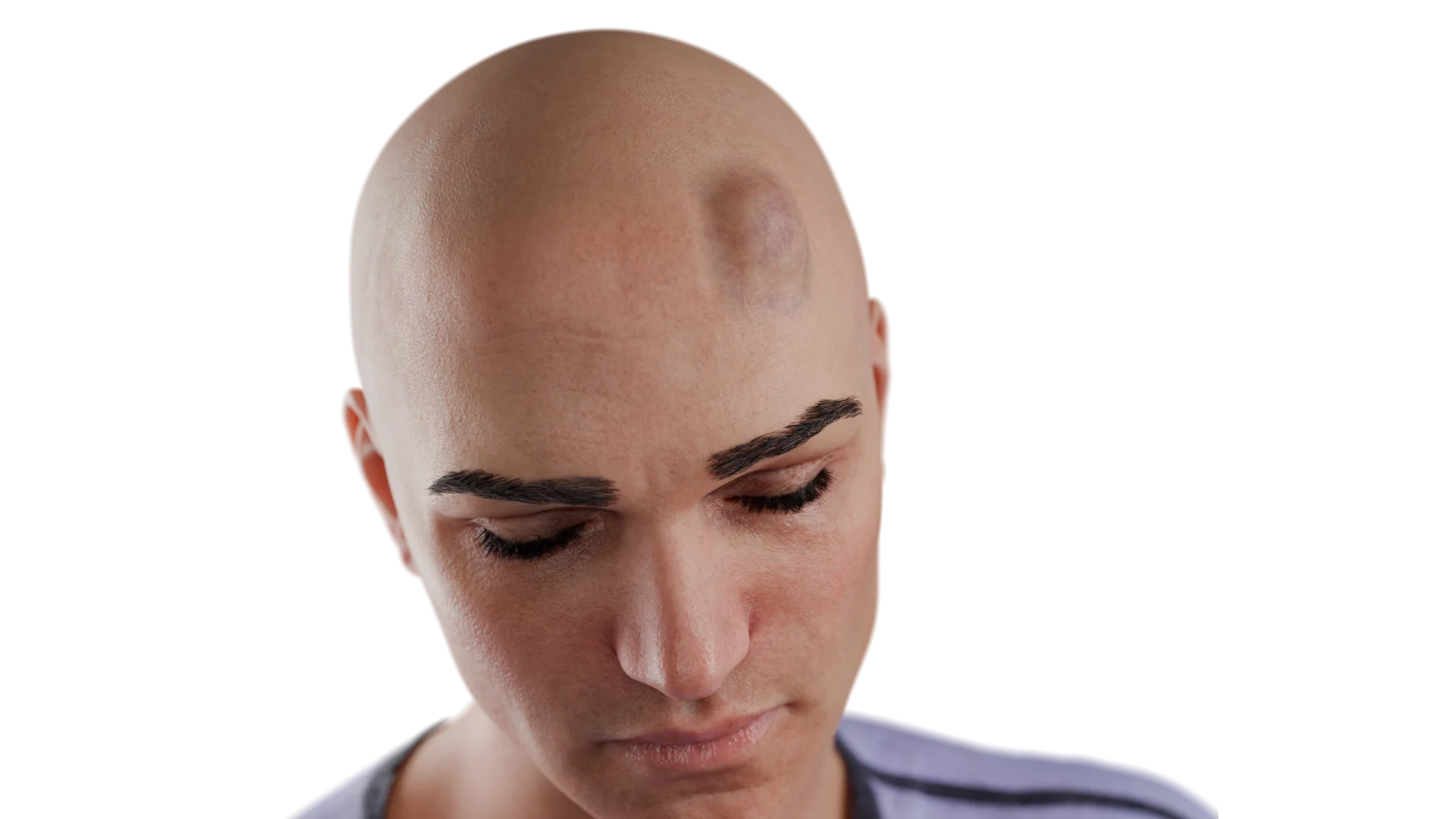
Examination of the patient allows to identify traces of head trauma (abrasions, hematomas, bruised wounds), which is extremely important for the differential diagnosis of traumatic brain injury with other emergency neurosurgical pathologies affecting the brain.
Examples of soft tissue injuries that can occur as a result of head injury are shown in 3D models.
A thorough examination also helps to rule out combined injuries, which are common in these patients and worsen the prognosis. The physician’s primary focus should be on the patient’s level of consciousness.
The level of consciousness of patients is commonly categorized into:
Clear consciousness;
Moderate stun;
Deep stun;
Sopore;
Coma (moderate, deep, inhibited).
Glasgow Consciousness Rating Scale (GCRS)
The Glasgow Coma Scale (GCS) is used in neurosurgery for rapid assessment of the level of consciousness to evaluate the patient’s condition in the emergency room and to decide on further treatment tactics. The GCS has a direct correlation with mortality: if the level of consciousness of a trauma patient is between 3 and 8 points, the mortality rate is about 60%.
The Glasgow Coma Scale includes assessment of 3 integral measures: motor response, eye opening, and verbal contact.
Eye opening (E, Eye response)
Spontaneous – 4 points;
On speech, 3 points;
For painful irritation, 2 points;
No response – 1 point.
Verbal response (V, Verbal response)
The patient is oriented, the answer to the question asked is correct and quick – 5 points;
Patient disoriented, confused speech – 4 points;
A verbal sprinkle, the answer does not correspond to the question in terms of meaning – 3 points;
Unintelligible sounds in response to a given question – 2 points;
Absence of speech response – 1 point.
Motor response (M, Motor response)
Execution of movements on command – 6 points;
Purposeful movement in response to painful stimulus (repulsion) – 5 points;
Limb jerking in response to painful stimulus – 4 points;
Pathologic flexion in response to painful stimulus – 3 points;
Pathologic extension in response to painful stimulus – 2 points;
Lack of motor reaction – 1 point.
The total sum of scores on the SCS ranges from 3 to 15. This scale allows to interpret a quantitative criterion (score) into a qualitative criterion (level of consciousness):
15 points – clear consciousness of the patient;
14-12 points – moderate stun;
11-10 points – deep stun;
9-8 points – soporus;
7-6 points – moderate coma;
5 to 4 is a deep coma;
3 points is a prohibitive coma.
Laboratory tests
Laboratory tests for traumatic brain injury (traumatic brain injury) include standard tests:
General blood count (GBC);
Biochemical blood count (BAC);
Coagulogram;
Urinalysis (OAM);
Determination of blood group and Rh factor.
These tests are performed not only to establish a diagnosis, but also to assess the patient’s condition, identify comorbidities, and prepare for possible surgical intervention.
Instrumental methods of diagnosing traumatic brain injury
Instrumental methods for diagnosing a traumatic brain injury include:
Computed tomography (CT): Recognized as the gold standard in the diagnosis of traumatic brain injury, this technique can detect skull bone fractures, brain contusions, intracerebral hematomas, and pathologic changes in the airway cavities. Advantages of CT include high speed of performance and high sensitivity and specificity. It is also possible to determine the age of injury by indirect signs on CT. CT is used in different variations (native CT examination, CT angiography, CT cisternography).
Our 3D Models show fractures of the skull vault and skull base that can be visualized with CT scans.
Fracture of the left temporal bone with transition to the temporal bone pyramid – 3D Model
Magnetic resonance imaging (MRI): Although more expensive and time-consuming to perform, MRI has advantages over CT. It allows better visualization of soft tissue and brain tissue without subjecting the patient to radiation exposure. MRI is effective for detecting intracranial hematomas at different stages of their development, brain damage and is the preferred method for diagnosing diffuse axonal damage. MRI also allows a more accurate assessment of liquor dynamics due to special programs, but is less effective in detecting traumatic injuries of the skull bones. MRI is performed in different programs (T1, T2 FLAIR, ADC, DWI, TOF etc.).
Lumbar puncture: This ancillary technique can detect the presence of subarachnoid hemorrhage, measure cerebrospinal fluid pressure and rule out complications of traumatic injury such as meningitis, meningoencephalitis and ventriculitis. Lumbar puncture can also be therapeutic in nature, allowing for liquor sanation and intrathecal administration of drugs.
Neuroendoscopic techniques: These techniques help to exclude occult liquorrhea and intraoperatively revise the natural spaces to detect ongoing hemorrhage.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment for brain injuries
Therapy of craniocerebral injury (CCI) is determined by the severity, clinical features, the patient’s level of consciousness and the presence or absence of cerebral edema. Treatment methods are divided into conservative and operative.
Conservative treatments for traumatic brain injury
Conservative therapy for traumatic brain injury is usually symptomatic and aims to control cerebral edema, control intracranial pressure, and eliminate symptoms.
The main groups of drugs are:
Non-steroidal anti-inflammatory drugs (NSAIDs): Used for pain management in conscious patients.
Antibiotics: Different groups and generations of antibiotics (β-lactams, aminoglycosides, macrolides, etc.) are used to prevent suppurative complications in patients with open or penetrating trauma and in patients with post-traumatic purulent meningitis. Antibiotics can be administered systemically, intrathecally or intraventricularly. An important property is their high permeability across the blood-brain barrier (BBB).
Anticonvulsants: Carbamazepine and valproic acid are used to prevent seizures in patients with focal brain damage.
Osmotic diuretics: Sorbitol and mannitol are used to control cerebral edema in severe traumatic brain injury. Loop diuretics such as furosemide may be used in combination.
Barbiturates: Used in conjunction with controlled hypothermia and artificial hypercapnia to reduce intracranial pressure.
Operative methods of treatment for traumatic brain injury
Surgical intervention is aimed at eliminating the factors causing acute or chronic compression of the brain. The tactics of surgical treatment depends on the patient’s level of consciousness, the history of injury and neuroimaging data.
Methods of surgical treatment:
Decompressive hemicraniectomy: It is used in severe traumatic brain injury patients to eliminate brain compression and prevent edema and dislocation.
Craniotomy with autocranioplasty: In acute cerebral compression in conscious patients, the substrate causing the compression is removed, followed by one-stage autocranioplasty.
Subdural drainage: In cases of chronic brain compression (e.g., chronic subdural hematomas), one or two milling holes are made and the hematomas are emptied and a closed drain is placed.
In patients with extremely severe traumatic brain injury and a level of consciousness on the Glasgow Coma Scale (GCS) of 3 points (terminal coma), surgical treatment is contraindicated due to high lethality and profound disability. Thus, the treatment of craniocerebral trauma requires a comprehensive approach, including both conservative and surgical methods, depending on the patient’s condition and features of trauma.
FAQ
1. What is a brain injury?
A craniocerebral injury is damage to the bones of the cranial vault or skull base, as well as to the brain itself, resulting from the impact of external mechanical factors on the head region.
2. What is the global prevalence of brain injury?
Approximately 27 million new cases of brain injury are reported worldwide each year (approximately 400 cases per 100,000 population). The mortality rate is about 10 per 100,000 population, with 70% of patients dying before receiving medical attention.
3. What are the main causes of brain injury ?
The most common causes of traumatic brain injury are: falls (40-50% of all head trauma cases), traffic accidents (20-30% of all head trauma cases), intentional bodily injury, and industrial injuries.
4. What are the main pathogenetic mechanisms of brain injury formation?
Two types of primary brain injury are distinguished – focal and diffuse. Focal ones are caused by the shock-impact mechanism (e.g., cerebral contusions, intracranial hematomas). Diffuse ones are associated with the acceleration-deceleration mechanism (concussion, diffuse axonal injury).
5. How is brain injury categorized by severity?
The severity of traumatic brain injury is divided into: mild traumatic brain injury (13-15 points on the Glasgow Coma Scale), moderate traumatic brain injury (9-12 points on the Glasgow Coma Scale) and severe traumatic brain injury (3-8 points on the Glasgow Coma Scale).
6. What symptoms occur in brain injury?
A variety of symptoms can occur with brain injury, including loss of consciousness, which can last from a few seconds to several weeks. Cerebral symptoms include headache, vomiting, and dizziness. Focal neurologic symptoms such as paresis, aphasia, and visual disturbances may also occur. Stem symptoms include oculomotor disorders and bulbar syndrome. Meningeal signs, such as occipital muscle rigidity, may also suggest brain injury.
7. What are the main methods of diagnosis of head injury?
The main methods for diagnosing head injury are visual examination of the patient to look for signs of traumatic injury to the soft tissues of the head. The patient’s level of consciousness is also assessed using the Glasgow Coma Scale. An important stage is the assessment of neurologic status, including the presence of general cerebral, focal and meningeal symptoms. Computed tomography (CT) is the gold standard in the diagnosis of skull fractures and detection of intracranial hematomas. Magnetic resonance imaging (MRI) is effective in assessing the extent of soft tissue damage to the head and brain, and in confirming the diagnosis of diffuse axonal injury. Lumbar puncture can be used to confirm traumatic subarachnoid hemorrhage.
8. What treatments are used for head injury?
Craniocerebral trauma is treated both conservatively and surgically. Conservative therapy includes the use of non-steroidal anti-inflammatory drugs for pain relief and reduction of inflammation. Antibiotics are also prescribed to prevent infectious complications, osmotic diuretics to control cerebral edema, and anticonvulsants to manage and prevent seizures. In cases of severe lesions requiring surgical intervention, decompressive hemicraniectomy is performed for unresectable malignant cerebral edema. Craniotomy with autocranioplasty may be performed to remove a focus of cerebral compression. Subdural drainage may be indicated to treat chronic brain compression.
9. What is the difference between a traumatic brain injury and a concussion?
A traumatic brain injury (traumatic brain injury (traumatic brain injury) includes all types of brain injuries, from mild to severe. A concussion is one of the mildest forms of traumatic brain injury, usually does not cause long-term damage and has no visible changes on imaging, unlike more serious injuries such as hematomas or skull fractures.
10. What is the most dangerous traumatic injury?
The most dangerous is a traumatic brain injury, with severe injuries such as open head injuries, massive hematomas, skull fractures, and brain stem injuries that can lead to respiratory or cardiac arrest.
11. How long does a brain injury last?
The duration of the traumatic process depends on the extent of the injury and the type of injury. Mild forms such as a concussion can last a few days, while more severe forms with hematomas or fractures require long-term treatment, sometimes months or even years.
12. Is it possible to recover 100% from a brain injury?
Recovery depends on the extent of the brain injury. In cases of mild injuries, recovery may be complete. However, in more serious cases, such as injuries that cause damage to brain tissue or structures, full recovery may not be possible and the effects may remain for life.
13. What are the consequences after a traumatic brain injury?
After a brain injury, there are various possible outcomes such as chronic headaches, memory problems, impaired coordination, personality changes, depression, seizures, visual or hearing impairment, and other neurological disorders.
14. How long do people live after a traumatic brain injury?
The prognosis for survival after a traumatic brain injury depends on the severity of the injury. Mild injuries usually do not affect life expectancy, whereas severe brain injuries can lead to death or serious long-term impairment.
15. How is rehabilitation after a traumatic brain injury?
Rehabilitation after a traumatic brain injury includes physical therapy, neuropsychological rehabilitation, restoration of cognitive functions and support of the patient’s psycho-emotional state. Recovery time depends on the extent of the injury and the patient’s condition, and can last from several months to several years.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Brazinova A, Rehorcikova V, Taylor MS, Buckova V, Majdan M, Psota M, Peeters W, Feigin V, Theadom A, Holkovic L, Synnot A. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J Neurotrauma. 2021 May 15;38(10):1411-1440. doi: 10.1089/neu.2015.4126. Epub 2018 Dec 19. PMID: 26537996; PMCID: PMC8082737.
3.
Esterov D, Bellamkonda E, Mandrekar J, Ransom JE, Brown AW. Cause of Death after Traumatic Brain Injury: A Population-Based Health Record Review Analysis Referenced for Nonhead Trauma. Neuroepidemiology. 2021;55(3):180-187. doi: 10.1159/000514807. Epub 2021 Apr 9. PMID: 33839727; PMCID: PMC8217128.
4.
Ng SY, Lee AYW. Traumatic Brain Injuries: Pathophysiology and Potential Therapeutic Targets. Front Cell Neurosci. 2019 Nov 27;13:528. doi: 10.3389/fncel.2019.00528. PMID: 31827423; PMCID: PMC6890857.
5.
Клиническое руководство по черепно-мозговой травме / под ред. А.Н. Коновалова, Л.Б. Лихтермана, А.А. Потапова. – М.: Антидор, 1998. – Т. 1. – 54 с.
6.
Rauchman SH, Zubair A, Jacob B, Rauchman D, Pinkhasov A, Placantonakis DG, Reiss AB. Traumatic brain injury: Mechanisms, manifestations, and visual sequelae. Front Neurosci. 2023 Feb 23;17:1090672. doi: 10.3389/fnins.2023.1090672. PMID: 36908792; PMCID: PMC9995859.
7.
Nelson LD, Temkin NR, Barber J, et al. Functional Recovery, Symptoms, and Quality of Life 1 to 5 Years After Traumatic Brain Injury: Findings From the TRACK-TBI Study. JAMA Netw Open. 2023;6(3):e233660. doi:10.1001/jamanetworkopen.2023.3660.
8.
Valko PO, Gavrilov YV, Yamamoto M, Noaín D, Reddy H, Haybaeck J, Weis S, Baumann CR, Scammell TE. Damage to Arousal-Promoting Brainstem Neurons with Traumatic Brain Injury. Sleep. 2016 Jun 1;39(6):1249-52. doi: 10.5665/sleep.5844. PMID: 27091531; PMCID: PMC4863213.
La Russa R, Maiese A, Di Fazio N, Morano A, Di Bonaventura C, De Matteis A, Fazio V, Frati P, Fineschi V. Post-Traumatic Meningitis Is a Diagnostic Challenging Time: A Systematic Review Focusing on Clinical and Pathological Features. Int J Mol Sci. 2020 Jun 10;21(11):4148. doi: 10.3390/ijms21114148. PMID: 32532024; PMCID: PMC7312088.
11.
Teasdale, G., & Jennett, B. (1974). ASSESSMENT OF COMA AND IMPAIRED CONSCIOUSNESS. The Lancet, 304(7872), 81–84. doi:10.1016/s0140-6736(74)91639-0.
12.
Клиническое руководство по черепно-мозговой травме / под ред. А.Н. Коновалова, Л.Б. Лихтермана, А.А. Потапова. – М.: Антидор, 1998. – Т. 1. –67 с.
13.
Schweitzer, A. D., Niogi, S. N., Whitlow, C. J., & Tsiouris, A. J. (2019). Traumatic Brain Injury: Imaging Patterns and Complications. RadioGraphics, 39(6), 1571–1595. doi:10.1148/rg.2019190076
14.
Lee H, Yang Y, Xu J, Ware JB, Liu B. Use of Magnetic Resonance Imaging in Acute Traumatic Brain Injury Patients is Associated with Lower Inpatient Mortality. J Clin Imaging Sci. 2021 Oct 4;11:53. doi: 10.25259/JCIS_148_2021. PMID: 34754593; PMCID: PMC8571198.
15.
Role of Lumbar Puncture In Traumatic Brain Injury. (2021). Indian Journal of Public Health Research & Development, 12(2), 308-311.
https://doi.org/10.37506/ijphrd.v12i2.14137
16.
Tanaka T, Liu X, Momozaki N, Honda E. Endoscopic-assisted removal of bilateral traumatic intracerebral hemorrhage: A case report. Surg Neurol Int. 2023 Aug 11;14:288. doi: 10.25259/SNI_268_2023. PMID: 37680938; PMCID: PMC10481816.
17.
Jha S, Ghewade P. Management and Treatment of Traumatic Brain Injuries. Cureus. 2022 Oct 23;14(10):e30617. doi: 10.7759/cureus.30617. PMID: 36426314; PMCID: PMC9681696.
18.
Fong, R., Konakondla, S., Schirmer, C. M., & Lacroix, M. (2017). Surgical interventions for severe traumatic brain injury. Journal of Emergency and Critical Care Medicine, 1(10), 28–28. doi:10.21037/jeccm.2017.09.03.