Basic Monitoring During Anesthesia: Standards and Mandatory Monitoring Parameters
Analysis of basic monitoring standards during anesthesia. Mandatory parameters of oxygenation, ventilation, and hemodynamics for patient safety.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Spinal, or subarachnoid anesthesia (SA), is a method of neuraxial anesthesia in which a local anesthetic (with or without adjuvants) is injected into the lumbar cerebrospinal fluid to achieve a predictable sensory and motor block by acting on the spinal nerve roots and spinal structures stemming from the spinal cord. Spinal anesthesia is used for achieving anesthesia and/or analgesia during various interventions on the spine, lower abdomen, pelvis, perineum, and lower extremities.
Spinal anesthesia can be used as a sole method or in conjunction with general anesthesia (GA) for procedures on the lower half of the body:
Spinal anesthesia (SA) is not only a “puncture technique” but primarily a managed intervention into the autonomic and conductive body pathways. Understanding the functional anatomy of the spine, the meninges, and the subarachnoid space, as well as the physiological effects of sympathetic, sensory, and motor blocks, allows for prediction of block spread and complication prevention. Operator’s anatomical and physiological literacy is directly related to the patient safety and predictability of their outcomes.
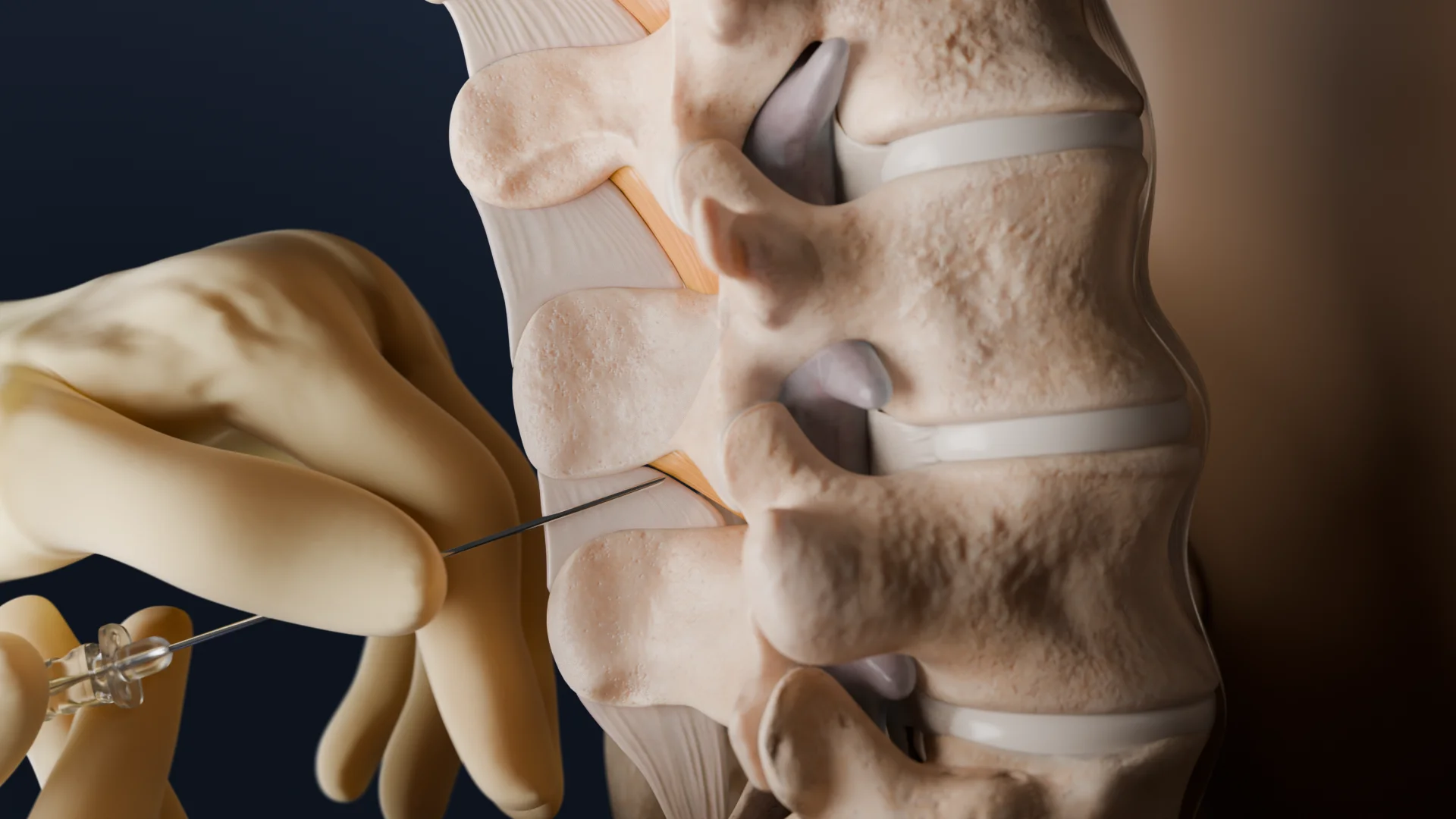
Performing spinal anesthesia requires the operator to have knowledge of the functional anatomy of the spinal block, which is impossible without deep knowledge of the structure of the spine, spinal cord, and spinal nerves.


1. Skin;
2. Subcutaneous adipose tissue;
3. Supraspinal ligament;
4. Interspinal ligament;
5. Ligamenta flava;
6. Dura mater;
7. Subdural space;
8. Arachnoid mater;
9. Subarachnoid space.
1. Skin;
2. Subcutaneous adipose tissue;
3. Paraspinal muscles;
4. Ligamenta flava;
5. Dura mater;
6. Subdural space;
7. Arachnoid mater;
8. Subarachnoid space.
SA induces a block of sympathetic, sensory, and motor fibers, compensatory reflexes, and vagotonia. From a clinical point of view, it is important that the level of sympathetic block usually exceeds the level of sensory one; therefore, hemodynamic changes may occur earlier and be more significant than expected based on the level of skin sensitivity.
Hypotension and bradycardia are the most common and significant physiological effects of neuraxial anesthesia, resulting from sympathetic block.
Sympathetic nerve block causes hypotension by affecting preload, afterload, contractility, and heart rate. In other words, a decrease in systemic vascular resistance and reduced venous return lead to hypotension.
Additional risk factors for the development of hypotension include pregnancy, pre-existing hypovolemia and blood loss, age over 40, obesity, chronic alcohol consumption, and hypertension.
The heart rate due to SA can increase (as a result of hypotension) or decrease (due to sympathetic fiber block, decreased venous return, the so-called Bainbridge reflex, and also as a result of the Bezold-Jarisch reflex, that is, the stimulation of left ventricular mechanoreceptors).
Risk factors for bradycardia include younger age, a heart rate less than 60 bpm, ASA class I, beta-blocker therapy, and a prolonged PR interval on the ECG.
In patients with normal lung function, spinal anesthesia affects it to the minimal extent. Minute ventilation (MV), dead space volume, shunt fraction, and arterial blood gases change insignificantly.
With a high spinal block, exhalation may be difficult due to paralysis of the intercostal and chest muscles (maximum MV and expiratory reserve volume are reduced). Therefore, patients with obstructive lung diseases, who require auxiliary muscles for adequate ventilation, should be monitored more closely after spinal block. Patients with normal lung function may complain of dyspnea in the event of a high spinal block (most often due to the inability to feel chest movement during breathing; describing the situation to the patient helps to ease their symptoms).
Since high SA does not usually affect the cervical spine, the function of the phrenic nerve and diaphragm is preserved.
Arterial blood gases do not change during high SA in patients breathing spontaneously at room temperature.
Vasodilation and decreased systemic vascular resistance lead to increased heat loss and shivering, which require active methods of warming the patient (external warming and the use of heated intravenous fluids), as during general anesthesia.
The practical sequence of the procedure includes the following steps:
Sitting and side-lying positions with maximum lumbar flexion are used, the choice of which depends on the physician’s preference, the planned position of the patient during the surgical procedure, the patient’s constitution, and their comfort. The physician may perform the procedure while sitting or standing. The prone jack-knife position (lying prone on the abdomen with bent legs) is used in rare cases during proctological or perineal surgeries. For these procedures, it is preferable to use a hypobaric or isobaric solution of local anesthetic.
The skin is treated with an antiseptic solution (e.g., 0.5% chlorhexidine). The solution must dry completely before continuing with the procedure.
A small amount of local anesthetic (1% lidocaine solution) is injected into the target puncture site to infiltrate the skin and subcutaneous tissue.
Preoperative ultrasound examination of the patient is recommended if there are difficulties palpating anatomical landmarks.
Using small-diameter needles (24-27 G) and needles with rounded, non-cutting bevels reduces the incidence of post-puncture headache.
With midline access, the guide needle is inserted at a slight cranial angle until denser tissue is felt, indicating that the tip of the needle is in the interspinal ligament.
Next, the spinal needle is inserted into the guide-needle. The needle passes through the ligamentum flavum, then the epidural space, and finally the dura mater. As the needle passes through each of these layers, a change in resistance is felt. A “pop” is often felt when piercing the dura mater. In patients with normal constitution, the depth of needle penetration from skin to dura mater is 5.0±1.0 cm.
After the “pop” or loss of resistance, the stylet should be removed, and if the maneuver is correctly performed, cerebrospinal fluid (CSF) will begin to flow through the needle tip. Outflow through smaller-diameter needles may be very slow, especially if the patient is in a side-lying position.
If there is no outflow, as the needle may be blocked by a nerve root, rotate the needle 90°.
Once free CSF outflow is ensured, slowly inject the local anesthetic at a rate of no more than 0.5 ml/sec. After completing the injection, the introducer and spinal needle are removed from the patient’s back.
Spinal anesthesia is usually administered as a single injection. Continuous spinal anesthesia via a catheter placed in the subarachnoid space is no longer used due to the frequency of neurological complications (cauda equina syndrome) and the high risk of post-puncture headache.
This includes assessment of sensory and motor blocks, as well as readiness to manage potential side effects such as hypotension and bradycardia.
If necessary, sedatives should be used to achieve the optimal effect in order to reduce patient anxiety, considering the direct sedative effect resulting from SA.
In SA, local anesthetics and adjuvants should be chosen to achieve the required level of spinal anesthesia and provide the necessary duration of anesthesia for the duration of the surgical procedure.
The most important factors determining the degree of sensory block are the dose and baricity (the ratio of the density of the solution to the density of cerebrospinal fluid; anesthetics are divided into hyperbaric, isobaric, and hypobaric) of the anesthetic solution.
Baricity affects the distribution of the anesthetic solution in the subarachnoid space: hyperbaric solutions tend to “sink” within the CSF relative to the injection site, while hypobaric solutions rise above the injection site.
Hyperbaric solutions result in a faster onset of action, greater sensory block, and shorter duration of action compared to isobaric solutions. It’s important to note that local anesthetics can be neurotoxic at higher concentrations.
Intrathecal opioids specified below may be added to improve intraoperative and postoperative analgesia.
α2-agonists enhance sensory and motor blocks, prolong duration of action, and promote postoperative analgesia by acting on alpha-adrenergic receptors in the spinal cord. Please see some examples below:
Find more scientifically accurate content on our social media








Expected complications include hypotension and bradycardia due to sympathetic block, nausea (hence prophylaxis with antiemetics is advised), patient discomfort due to motor and sensory block, as well as shivering.
1. What is spinal anesthesia?
2. How long does the effect of spinal anesthesia last?
3. How long does it take for full recovery after the procedure?
4. How does spinal anesthesia differ from epidural anesthesia?
5. Which surgeries are most commonly performed under spinal anesthesia?
6. What are the absolute contraindications for performing spinal anesthesia?
7. Which agents are most commonly used?
8. Why does hypotension occur after spinal anesthesia?
9. What is a “high” or “total” spinal block?
10. What is a post-dural puncture headache, and how to reduce the risk of its occurrence?
11. What are transient neurological symptoms (TNSs), and how are they different from serious complications?
12. What postoperative symptoms require immediate attention?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Ledesma I., Stieger A., Luedi M.M. (2024). Spinal anesthesia in ambulatory patients. Curr Opin Anaesthesiol. 37(6):661-665. doi: 10.1097/ACO.0000000000001412.
3.
DeLeon A.M., Wong C.A. Spinal anesthesia: Technique. In: Post TW, ed. UpToDate [Internet]. Waltham (MA): UpToDate; 2025 [updated 2025 Jun 26; cited 2026 Jan].
4.
Kietaibl S., Ferrandis R., Godier A. (2022). Regional anaesthesia in patients on antithrombotic drugs. European Journal of Anaesthesiology 39(2):p 100-132. DOI: 10.1097/EJA.0000000000001600.
Loading test 6 questions
Table of Contents
Related articles




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io