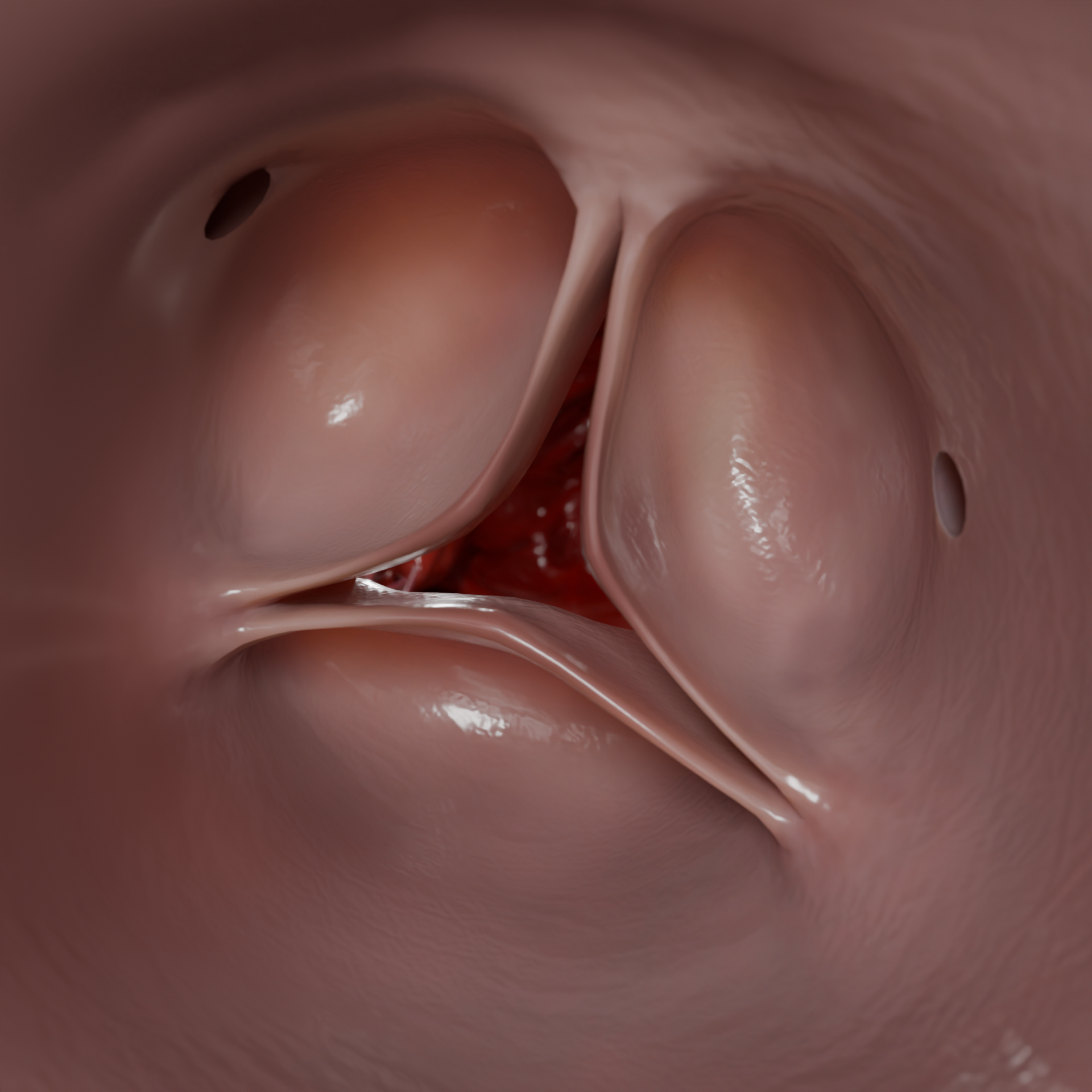
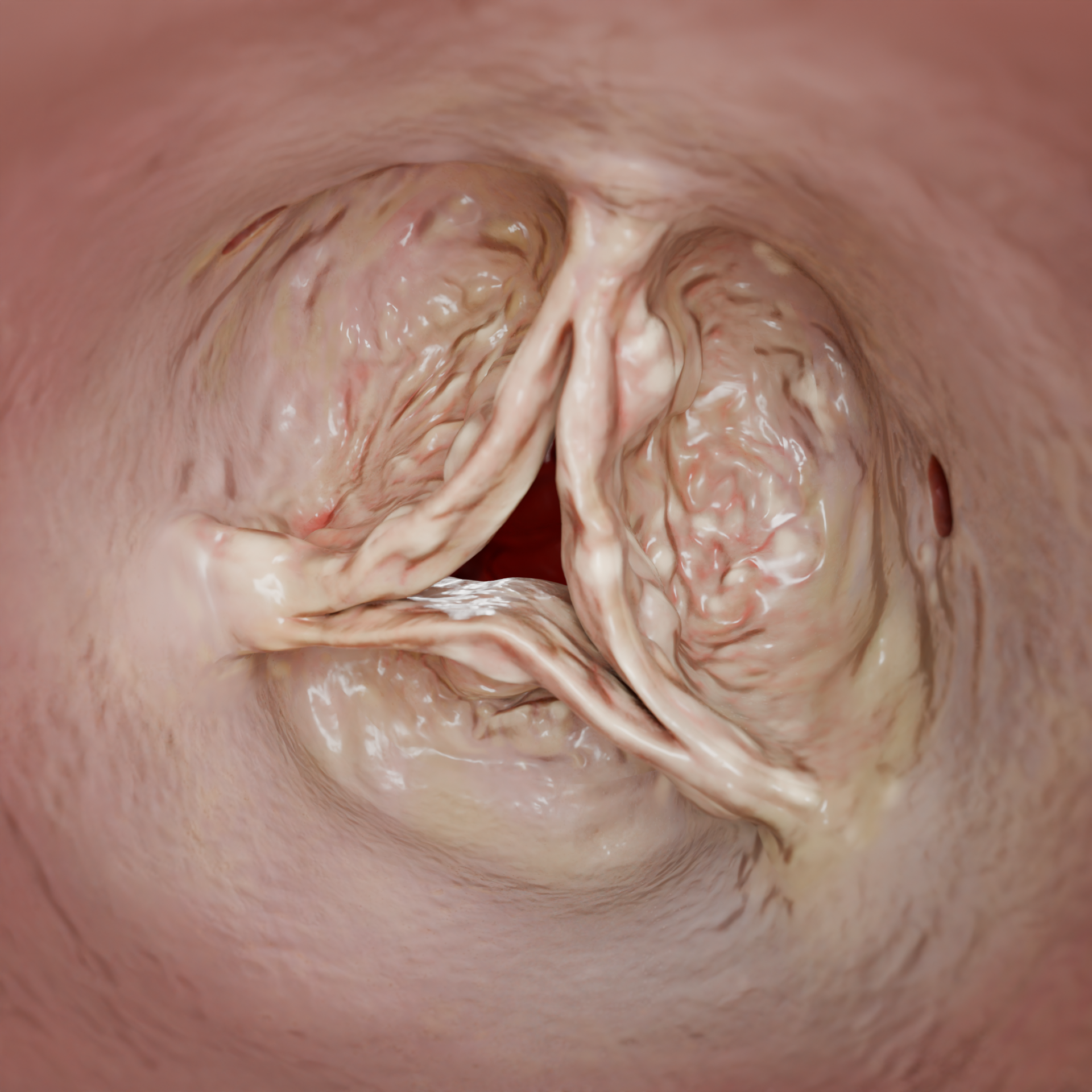
Aortic regurgitation (AR) is a heart disease when the leaflets of the aortic valve (AV) do not close properly, resulting in reversed blood flow (regurgitation) from the aorta into the left ventricle (LV).3D Animation: Aortic Valve Dilatation3D Animation: Aortic Valve Leaflet Redundancy
Epidemiology
AR is among the three most common valvular heart diseases worldwide. According to the Framingham Heart Study, its prevalence among adults amounts to 4.9 %, with moderate to severe cases occurring in 0.5 % of patients.
Moreover, males are more prone to AR than females.
In developed countries, the primary drivers of AR are age-related, degenerative, and atherosclerotic alterations of the valve.
In countries with limited access to adequate medical care, the primary causes of AV damage shift to infections, such as rheumatic fever and infective endocarditis. These conditions can lead to early-onset aortic regurgitation (AR), often manifesting in childhood.
Over the coming decades, the AR burden is expected to rise due to aging populations and ever-increasing prevalence of cardiovascular conditions. Additionally, advances in echocardiographic (ECG) studies have allowed healthcare professionals to detect more asymptomatic AR cases, improving early diagnosis and intervention.
Annular Dilatation – 3D ModelExcessive Leaflet Tissue – 3D Model
Etiology
Degenerative processes, including calcification, fibrosis, and leaflet prolapse, often develop alongside aortic stenosis (AS). Infective endocarditis may destroy the leaflets, while rheumatic fever leads to deformation and progressive regurgitation.
Systemic connective tissue disorders (Marfan syndrome, Loeys — Dietz syndrome, vascular Ehlers — Danlos syndrome) are associated with aortic dilation and a high risk of aortic dissection. Inflammation (Takayasu arteritis, granulomatosis with polyangiitis) and autoimmune diseases (systemic lupus erythematosus, antiphospholipid syndrome) tend to remodel the aorta and give rise to secondary AR.
AV annular dilation induced by aneurysms, hypertension, and connective tissue disorders, results in leaflet separation. Leaflet prolapse and excessive leaflet tissue prevent the leaflets from closing properly, further exacerbating regurgitation.
AR may also be detected in cases of paravalvular leaks following replacement surgery.
Rheumatic Aortic Stenosis – 3D ModelDegenerative Aortic Stenosis – 3D Model
Pathophysiology
Acute AR develops abruptly and is frequently associated with infective endocarditis, aortic dissection, or leaflet trauma.
Acute volume overload and diastolic pressure increase: Excessive blood that flows back into the LV during diastole triggers rapid increase in end diastolic pressure (EDP). Eventually, LV compliance is reduced, the left atrium (LA) becomes overloaded, and pulmonary circulation congestion develops, ultimately resulting in pulmonary edema.
Reduced effective cardiac output: Despite a hyperdynamic LV, a large volume of blood returns to its cavity, leading to blood pressure drop, organ hypoperfusion, and cardiogenic shock.
Disruption in coronary perfusion: Elevated EDP in the LV reduces the pressure gradient between the aorta and coronary arteries. This further reduces blood supply to the myocardium and triggers ischemia.
Compensatory reaction: The sympathoadrenal system is activated causing tachycardia and vasoconstriction in an attempt to maintain cardiac output. However, this mechanism increases afterload and exacerbates regurgitation.
Acute AR is responsible for a rapid-onset pulmonary edema, hypotension, and cardiogenic shock, necessitating emergency surgical intervention.
Chronic AR develops gradually, frequently due to degenerative changes of the valve, bicuspid aortic valve, rheumatic fever, or aortic dilation. Initially, the heart adapts to the persistent overload; however, over time, compensatory mechanisms start to fail, ultimately leading to decompensated AR.
Eccentric LV hypertrophy: Prolonged volume overload dilates the LV and prompts myocyte growth to help maintain normal cardiac output.
Progressing LV dilation: In advanced stages, LV walls lose elasticity as the valvular volume becomes chronically enlarged. This reduces the ejection fraction (EF) and eventually causes systolic dysfunction. The LV end diastolic diameter exceeds 70 mm.
Coronary blood flow disruption: An enlarged LV has an increased oxygen demand. However, low diastolic pressure in the aorta compromises myocardial perfusion, which contributes to ischemia.
Hemodynamic changes: Low diastolic pressure (< 50 mmHg) reduces coronary blood flow, while chronic overload of the pulmonary circulation elevates pressure in the LA and pulmonary veins.
Cardiac failure: As the disease progresses, congestion develops in both the pulmonary and systemic circulations. The condition is accompanied by dyspnea, orthopnea, paroxysmal nocturnal dyspnea, as well as peripheral edema and hepatomegaly (enlarged liver).
Clinical Manifestations
Acute AR is linked to rapid aggravation of a patient’s condition.
Sudden dyspnea, that may evolve to pulmonary edema, often occurs alongside orthopnea and asphyxia.
Marked hypotension and cardiogenic shock are caused by acute drop in cardiac output. The symptoms include fatigue, dizziness, and impaired consciousness.
Sometimes, infective endocarditis may give rise to fever, chills, and signs of sepsis.
Chronic AR remains asymptomatic for long periods of time as the LV adapts to volume overload.
As the disease progresses, a patient starts to experience palpitations and increased pulse, particularly in a supine position. This is attributed to an increased stroke volume and high pulse pressure.
Patients may also complain about a pushing sensation in the region of head and neck, that is associated with stronger pulsation of the large arteries.
Over time, physical activity triggers dyspnea. Severe cases of AR are marked by persistent dyspnea, with nocturnal episodes indicative of congestion in the pulmonary circulation.
Some patients may experience heartaches that point to reduced coronary perfusion due to low diastolic pressure. Angina pectoris in AR typically occurs at night, when heart rate slows, further reducing coronary blood flow.
Advanced stages of the disease are characterized by exacerbated congestive cardiac failure, including peripheral edema, hepatomegaly (enlarged liver), and ascites (fluid buildup in the abdomen).
Diagnosis
Transthoracic echocardiogram (TTE): This is the key method to confirm AR, assess the AV morphology, regurgitation severity, the LV size and function, and the size of the aorta.
Signs of severe AR according to TTE: Vena contracta > 6 mm; reversed diastolic flow in the descending aorta. Regurgitation volume > 60 ml per cycle. Regurgitation fraction > 50 %. Effective regurgitant orifice area (EROA) ≥ 0.030 cm2.
TTE Assessment of AR Severity
Parameter
Mild AR (Grade I)
Moderate AR (Grade II)
Severe AR (Grade III)
Vena contracta diameter
3 mm
3-6 mm
> 6 mm
Regurgitation volume
30 ml
30-60 ml
60 ml
Regurgitation fraction
30%
30-50%
> 50%
Effective regurgitant orifice area (EROA)
0.10 cm²
0.10-0.30 cm²
≥ 0.30 cm²
Reversed diastolic flow
Absent
Present but not in the descending aorta
Reversed blood flow in the descending aorta
Transesophageal echocardiogram (TEE): This imaging modality is indicated if TTE has not been informative enough, particularly if infective endocarditis is suspected or surgery is considered.
Magnetic resonance imaging (MRI): Though rarely employed (especially when ECG is not informative), this method may help assess regurgitation volume and LV function.
Computed tomography (CT): This tool provides a detailed assessment of the aortic size and condition. It is especially useful when dilation or an aneurysm is suspected or a surgical approach is being chosen.
Echocardiogram (ECG): This technique is employed to identify any signs of LV hypertrophy and concomitant abnormalities.
Chest X-ray: A scan shows an enlarged heart and any signs of pulmonary engorgement.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Aortic Regurgitation Treatment
Risk Factor Modification
Blood pressure control: Systemic hypertension contributes to aortic root dilatation and impairs leaflet coaptation.
Hyperlipidemia treatment, abstinence from smoking, body weight management.
Regular moderate physical activity: It improves the functional status of the heart. However, marked AR is not compatible with high-intensity strength training or high-static sports (e.g., weightlifting).
Medical Therapy
Hypotensive therapy is employed to manage arterial hypertension and aortic dilation. Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers have proven to be the most effective, as they reduce afterload and LV dilation.
Beta-blockers or calcium channel blockers are preferred for patients with Marfan syndrome to slow aortic dilation.
To reduce cardiac load in congestive cardiac failure, diuretics may be used.
Beta-blockers are also utilized in aortic dilation. However, they are contraindicated in isolated severe AR without hypertension, as this therapy may adversely affect hemodynamics.
Vasodilators may be used with caution in certain cases of symptomatic AR accompanied by high vascular resistance.
Transcatheter Aortic Valve Implantation (TAVI)
Unlike in AS, the procedure is of limited use in patients with isolated AR. Restrictions are imposed by anatomical features: If leaflets are not calcified, the prosthesis is expected to be less stable, increasing the risk of paravalvular leaks and valve displacement.
Contraindications for TAVI in AR patients: Isolated AR with non-calcified leaflets; significant aortic root dilation, which compromises prosthesis stability.
3D Animation: Transcatheter Aortic Valve Implantation (TAVI)
Surgical Therapy
Surgery remains the primary treatment option for severe AR, especially in symptomatic patients or those presenting with signs of LV dysfunction.
Aortic valve replacement (AVR) may be indicated in the following cases:
Symptomatic severe AR
Asymptomatic severe AR (LV end diastolic dimension (EDD) 70 mm, end systolic dimension (ESD) 50 mm, or EF 50 %)
Ascending aortic surgery is performed in cases of marked aortic dilation ( 55 mm, 50 mm in patients with Marfan syndrome).
Both mechanical and biological valves may be utilized. The material is chosen based on the patient’s age, contraindications for anticoagulant therapy, and concomitant conditions.
3D Animation: Aortic Valve Replacement
Aortic Valvuloplasty and Valve-Sparing Procedures
Reconstruction surgery is an option for patients with AR caused by leaflet prolapse, local fibrous deformation, or aortic root dilation. The main valvuloplasty types include:
Leaflet resection and reefing: This method is used in cases of leaflet prolapse that is eliminated by leaflet shortening and fixation.
Leaflet reconstruction with autologous pericardium or animal pericardium: This procedure is selected when the leaflets are significantly deformed and need to be restored without valve replacement.
Valve-sparing surgery is preferred for younger patients, which helps them avoid lifelong anticoagulant therapy. However, the indications are limited, and the leaflets should be either normal or have minimal anatomical changes.
David procedure: The aortic valve is reimplanted into an artificial vascular prosthesis, securing the leaflets. This prevents separation in cases of aortic root dilation.
Yacoub procedure: The procedure involves remodeling of the aortic root; its dilated portion is replaced with a vascular prosthesis while the fibrous ring (anulus fibrosus) remains intact, preserving the patient’s aortic valve.
FAQ
1. What is AR?
AR is a heart disease when the leaflets of the aortic valve do not close properly, resulting in reversed blood flow from the aorta into the left ventricle during diastole.
2. Can AR be congenital?
Although AR is primarily an acquired condition, in rare cases it may be congenital. The disease may be associated with: • Bicuspid aortic valve (the most common congenital anomaly responsible for AR); • Leaflet developmental defects (incomplete closure due to shortened or deformed leaflets); • Connective tissue disorders (Marfan syndrome, Ehlers — Danlos syndrome), which may trigger dilation of the aorta and valvular region.
Congenital AR progresses slowly over time but requires regular monitoring. Eventually, surgery may be indicated.
3. What are the symptoms of AR?
Symptoms generally vary based on its type (acute or chronic) and severity: • Acute AR: Acute dyspnea, pulmonary edema, fatigue, hypotension, shock (urgent medical help is required); • Chronic AR:
Early stages: Often asymptomatic, though some patients may experience palpitations or pulsating sensations in the neck and head.
Progression: Symptoms may include dyspnea during physical activity, angina pectoris (due to reduced coronary blood flow), and nocturnal asthma attacks.
Decompensation: This stage is marked by edema, hepatomegaly, reduced tolerance to physical activity.
4. What are the findings of AR auscultation?
A diastolic blowing murmur is heard best at the right superior sternal border (intercostal space 2) with the patient sitting up and leaning forward.
5. What are the general recommendations for AR patients?
• Blood pressure control and adjustment to reduce LV load. • Regular check-ups: ECG to assess the disease progression (1–2 times per year). • Physical activity: Moderate exercise (walking, swimming) is encouraged, though heavy weight training should be avoided. • Endocarditis prevention: Preventive antibiotic therapy prior to dental/surgical procedures (if indicated). • Surgery: Cases when LV dysfunction has become symptomatic (EF < 50 %, EDD > 70 mm).
Note: While asymptomatic AR requires regular follow-up, the onset of symptoms should prompt consultation with a cardiologist to evaluate the need for surgery.
List of Sources
1.
2021 ESC/EACTS Guidelines for the management of valvular heart disease. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W; ESC/EACTS Scientific Document Group. Eur Heart J. 2022 Feb 12;43(7):561-632. doi: 10.1093/eurheartj/ehab395.
2.
Burden of valvular heart disease, 1990-2017: Results from the Global Burden of Disease Study 2017. Chen J, et al. J Glob Health. Sep 8;10(2):020404. doi: 10.7189/jogh.10.020404.
3.
Aortic Valve Regurgitation: A Comprehensive Review. Oluwaseun A. Akinseye MD, MPH Aradhana Pathak MD Uzoma N. Ibebuogu MD. Current Problems in Cardiology. 2018 Aug; 43(8):315-334. doi: 10.1016/j.cpcardiol.2017.10.004.
4.
TAVI and the future of aortic valve replacement. Howard C, Jullian L, Joshi M, Noshirwani A, Bashir M, Harky A. J Card Surg. 2019 Dec;34(12):1577-1590. doi: 10.1111/jocs.14226.
5.
Aortic Valve Repair for Aortic Insufficiency Due to Cusp Prolapse. David TE. Ann Thorac Surg. 2023. Feb;115(2):436. doi: 10.1016/j.athoracsur.2022.06.047.
6.
Aortic Regurgitation. Flint N, Wunderlich NC, Shmueli H, Ben-Zekry S, Siegel RJ, Beigel R. Curr Cardiol Rep. 2019 Jun 3;21(7):65. doi: 10.1007/s11886-019-1144-6.